Prevalence of ASA in newborn
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (172.44 KB, 4 trang )
Pediatr Cardiol 27:343–346, 2006
DOI: 10.1007/s00246-005-1224-9
Prevalence of Interatrial Septal Aneurysm in Newborns and Their Natural Course
N. Ozcelik,1 S. Atalay,2 E. Tutar, F. Ekici2
1
2
7710 Van Zandt Dr., Corpus Christin, Texas 78413, USA
Department of Pediatric Cardiology, Ankara University School of Medicine, Ankara, Turkey
Abstract. The objective of this study was to evaluate
the prevalence of atrial septal aneurysm (ASA) in
newborns, to define the natural course of ASA, and
to investigate its role on closure of associated interatrial septal opening (IASO). A total of 1072
consecutive neonates were examined with echocardiography in the early postnatal period. The length of
the interatrial septum, the diameter of IASO, the
excursion and base of aneurysm, and the width of the
related atrium were measured and the excursion ratio
and the basal ratio were calculated for each neonate.
Aneurysms with an excursion ratio ‡25% were diagnosed as ASA. There were 81 neonates (7.6%) with
ASA. The prevalence of ASA was 11.1% in preterm
(14 of 126) and 7.1% in full-term newborns (67 of
946). All of the ASAs disappeared at the end of the
first year of life, and there were no complications
related to the lesion during the follow-up period.
Although overall IASO prevalence was 78.6% (843 of
1072), it was 72.8% (59 of 81) among the cases with
ASA. Although the disappearence time of interatrial
septal shunt was not significantly different between
the cases with and without ASA, spontaneous closure
was less frequent in the cases with ASA than in those
without ASA 77.7 and 96.1%), respectively (p <
0.001). The prevalence of ASA is high among newborns, with a high resolution rate. Therefore, it can
be considered that it is benign and transient observation. Less frequent spontaneous closure of IASO in
cases with ASA indicates that ASA may have a deleterious effect on spontaneous closure.
Key words: Atrial septal aneurysm — Newborn
Atrial septal aneurysm (ASA) is a localized bulging of
the interatrial septum into the right, left, or both
atriums. The pathogenesis of the lesion is not wellknown. There are various complications related to
Correspondence to: N. Ozcelik, email:
ASA, and it is still debated whether the lesion is benign or not [11, 13, 18, 20]. Since a limited number of
studies have been conducted on ASA in children, the
incidence of ASA in childhood is not well-known.
The objectives of this study are to evaluate the
prevalence of ASA in newborns, to define the natural
course of the lesion, and to investigate the role of
ASA in closure of associated interatrial septal openings (IASOs).
Materials and Methods
Neonates who were born in the obstetric department of a university
hospital between May 2002 and May 2003 and for whom informed
consent was obtained from the parents were examined with twodimensional and color Doppler echocardiography (Model Sonos
5500, Hewlett Packard; 3.5- 8- to MHz multifrequency transducer)
24–72 hours postnatally. Newborns with major congenital heart
disease were not included in the study. All neonates were studied in
standard echocardiographic positions. Interatrial septum was
examined mainly in subcostal positions. The presence of aneurysmatic excursion of the interatrial septum and associated IASOs
with shunt confirmed by color Doppler echocardiography was
noted. The presence of other associated cardiac lesions was also
evaluated. With the use of two-dimensional echocardiography, the
length of the interatrial septum (IASL) and the diameter of IASO if
present were measured at the end of diastole in the subcostal
bicaval view. The maximum aneurysmatic excursion length from
the interatrial septum and the base length of the aneurysm were
measured at the subcostal four-chamber view (Fig. 1).
The ratio of excursion length of ASA to the width of the
related atrium, which is the maximum excursion seen through it
(excursion ratio) was calculated. The ratio of the base length of
ASA to the IASL (basal ratio) was also calculated. When the
excursion ratio was ‡25%, the lesion was diagnosed as an ASA [21].
The shape and the direction of motion of the aneurysm were noted.
After ASA was diagnosed, the first reassessment was done at 1
month of age. Then all cases were followed up in the first year of
life in 3 month intervals to evaluate the natural course of ASA.
Statistical analysis was done by using SPSS 11.0 for Windows.
Mann–Whitney U, Kruskal–Wallis and chi-square tests were used
for comparisons. In addition, to show correlations between the results, Pearson correlation analysis was used. All values are given as
mean (standard deviation) and p < 0.05 is accepted as significant.
344
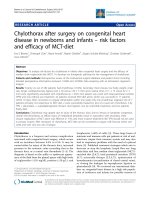
Fig. 1. Echocardiographic measurements of atrial septal aneurysm
(ASA). IASL, length of interatrial septum; LA, left atrium; RA,
right atrium; LV, left ventricle; RV, right ventricle.
Results
A total of 1075 consecutive neonates were evaluated
with echocardiography. Three neonates had major
congenital heart disease (tetralogy of Fallot, abnormal
left coronary artery originating from the pulmonary
artery, and transposition of the great arteries). These
patients were excluded. The study population consisted of 1072 newborns. Septal aneurysmatic excursion into the atria was seen in 101 newborns; 81 (7.6%)
of them qualified to have ASA. The mean gestational
age was 38.1 (2.0) weeks (range, 30–41) and the mean
birth weight was 3085 (627) g (range, 1050–4500).
Forty-one patients (50.6%) were male and 40 (49.4%)
were female. One hundred and twenty-six neonates
were preterm, with a gestational age of <37 weeks,
and 946 were full-term, with a gestational age of ‡37
weeks. The prevalence of ASA was not affected by
gender (p > 0.05) and was higher in preterm compared
to full-term neonates (11.1 and 7.1%, respectively;
p = 0.028). All ASAs were moving (56.8% into the
left, 3.7% into the right, and 39.5% into both atriums)
and all were hemispherical in shape. Echocardiographic measurements and calculations related to the
size of ASA are shown in Table 1.
Eight hundred and fourty-three of 1072 neonates
(78.6%) had IASOs. IASO was detected in 59 of 81
newborns with ASA (72.8%). The mean diameter of
IASO was not different between the patients with and
without ASA (3.51 ± 1.40 and 3.35 ± 1.12 mm,
respectively; p = 0.699). There were also no differences in excursion length, excursion ratio, base
length, and basal ratio of ASA between the patients
with ASA associated with and those without IASO
(Table 1).
Echocardiographic evaluation showed other
congenital heart defects that were also identified in
Pediatric Cardiology Vol. 27, No. 3, 2006
our study population, including isolated ventricular
septal defect (VSD) in 51, patent ductus arteriosus in
2, and bicuspid aortic valve in 5 patients. We found
that 4 of the 51 VSDs were associated with ASA.
Follow-up examinations were completed in 65
neonates with ASA. Septal aneurysm disappeared in
all cases. Aneurysm no longer existed in 69.2% (45 of
65) after 1 month and in 93.8% (61 of 65) after 3
months of age (Fig. 2). We found that there was no
correlation between disappearance time of ASA and
gestational age, birth weight (p > 0.05), and previously mentioned echocardiographic measurements
and calculations (Table 2).
Follow-up was completed in 509 patients with
IASO, consisting of 45 with ASA and 464 without
ASA. IASO closed spontaneously in 35 patients with
ASA (77.7%) and 446 patients without ASA (96.1%)
(p < 0.001). There was no difference in the closure
time of IASO between the two groups (p = 0.853).
Mean closure time of IASO was 3.7 (2.6) months in
patients with ASA and 3.6 (2.5) months in patients
without ASA. There were no complications related to
ASA during follow-up examinations.
Discussion
ASA is not usually clinically recognized but can be
easily diagnosed by cross-sectional echocardiography. Diagnostic criteria used for the diagnosis of
ASA in children are different from those for adults [8,
10]. As did Wolf et al. [21], we designated the lesion
as an ASA if the excursion ratio was ‡25%.
Different prevalences of ASA have been reported
for different age groups in various studies. This may
be due to both the criteria used for the diagnosis and
the age at which the patients were studied. The
accurate prevalence of ASA in the population is not
well defined. The prevalence has been reported to be
0.2–0.5%, 1.7–4.9%, and 26–64% for adults, children,
and fetuses, respectively [10, 14–17, 21]. The overall
high prevalence of ASA (7.6%) in this study and the
increased prevalence in preterm compared to fullterm infants (11. 1 vs 7.1%) indicate that the prevalence of ASA is clearly affected by gestational age
[4, 16].
ASAs are usually associated with additional
cardiac anomalies [1, 3, 4, 12, 14, 18]. The association
of ASA and interatrial septal-communication was
found to be 72.8% in our study, and this result is
comparable to previous reports [3–7, 18]. Guntheroth
et al. [9] reported that ASA is associated with small
patent foramen ovales, but we did not find any difference in the prevalence and diameter of IASOs
between the patients with and without ASA in our
study. Brand et al. [6] described that ASA may have a
Ozcelik et al.: Atrial Septal Aneurysm in Newborns
345
Table 1. Echocardiographic measurements and calculations in cases with ASA
Echocardiographic measurement
Mean (SD)
Upper–lower limits
Cases with
IASO (n = 59)
Cases without
IASO (n = 22)
p
IASL (mm)
Excursion length of ASA (mm)
Base length of ASA (mm)
Excursion ratio of ASA (%)
Basal ratio of ASA (%)
18.9
5.3
8.4
37.3
44.7
13.7–24.9
3.0–7.9
3.7–13.3
25.7–68.3
23.8–67.8
18.9
5.3
8.5
38.0
45.2
18.9
5.2
8.1
35.5
43.1
0.903
0.659
0.308
0.358
0.418
(2.0)
(1.1)
(2.1)
(9.2)
(10.4)
(2.2)
(1.1)
(2.1)
(9.6)
(10.5)
(1.7)
(1.0)
(1.8)
(8.0)
(9.9)
ASA, atrial septal aneurysm; IASL, length of interatrial septum; IASO, interatrial septal opening.
Fig. 2. Disappearence time of atrial septal
aneurysm (ASA) with Kaplan–Meier curve.
Table 2. Correlations between disappearance time of ASA and
echocardiographic measurements
Echocardiographic
measurement
Pearson correlation
coefficient (r)
p
IASL (mm)
Excursion length of ASA (mm)
Base length of ASA (mm)
Excursion ratio of ASA (%)
Basal ratio of AS A (%)
0.102
0.104
)0.048
)0.056
)0.069
0.426
0.410
0.708
0.656
0.588
was conducted on an unselected newborn population,
we believe that it gives a better estimate of the prevalence of ASA than those previously reported.
Regarding the high resolution rate, we believe that
ASA is a benign and transient lesion. Less frequent
spontaneous closure of IASO in the patients with
ASA indicates that aneurysms may have a negative
influence on spontaneous closure of IASOs, but more
studies are needed.
ASA, atrial septal aneurysm; IASL, length of interatrial septum.
role in spontaneous closure of associated IASO in
children, as have some other authors [2, 9, 15, 19]. On
the contrary, we found that although spontaneous
closure time of IASO was not different between two
groups, it was less frequent in patients with ASA.
Thus, our findings suggest that ASA may have a
deleterious effect on spontaneous closure of IASO.
Spontaneous recovery of ASA occurred in all of our
patients who completed 1 year of follow-up. This
finding is also supported by the fact that ASA is regressed and recovered in the course of time [4, 16, 21].
Conclusion
We found a high ASA prevalence (7.6%) among
newborns in this prospective study. Since our study
References
1. Arvan S (1986) Incidental interatrial septal aneurysm associated with mitral valve prolapse. Am Heart J 111:603–605
2. Awan IH, Rice R, Moodie DS (1982) Spontaneous closure of
atrial septal defect with interatrial aneurysm formation. Documentation by noninvasive studies, including digital substraction angiography. Pediatr Cardiol 3:143–145
3. Barbosa MM, Pena Motta MM, Fortes PR (1990) Aneurysms
of the atrial septum diagnosed by echocardiography and their
associated cardiac abnormalities. Int J Cardiol 29:71–78
4. Baysal K, Belet N, Kolbakır F, Yalın T (2001) Atrial septal
aneurysm in children. Turk J Pediatr 43:293–297
5. Belkin RN, Waugh RA, Kisslo J (1986) Interatrial shunting in
atrial septal aneurysm. Am J Cardiol 57:310–312
6. Brand A, Keren A, Branski D, Abrahamov A, Stern S (1989)
Natural course of atrial septal aneurysm in children and the
potential for spontaneous closure of associated septal defects.
Am J Cardiol 64:996–1001
346
7. Fox ER, Picard MH, Chow CM, et al. (2003) Interatrial septal
mobility predicts larger shunts across patent foramen ovales:
an analysis with transmitral Doppler scanning. Am Heart J
145:730–736
8. Gallet B, Malergue MC, Adams C, et al. (1985) Atrial septal
aneurysm—a potential cause of systemic embolism: an echocardiographic study. Br Heart J 53:292–297
9. Guntheroth WG, Schwaegler R, Trent E (2004) Comparative
roles of the atrial septal aneurysm versus patent foramen ovale
in systemic embolization with inferences from neonatal studies.
Am J Cardiol 94:1341–1343
10. Hanley PC, Tajik AJ, Hynes JK, et al. (1985) Diagnosis and
classification of atrial septal aneurysm by two-dimensional
echocardiography: report of 80 consecutive cases. J Am Coll
Cardiol 6:1370–1382
11. Kirk R (1996) Atrial septal aneurysm in children. Circulation
93:398
12. Magherini A, Margiotta C, Bandini F, Simonetti L, Bartolozzi
G (1986) Atrial septal aneurysm, ectasia of Valsalva and mitral
valve prolapse in Marfan’s syndrome. Am J Cardiol 58:172–173
13. Miga D, Case CL, Gillette PC (1996) Interatrial septal aneurysms and atrial arrhythmias in infants. Am Heart J 132:776–778
Pediatric Cardiology Vol. 27, No. 3, 2006
14. Rice MJ, McDonald RW, Reller MD (1988) Fetal atrial septal
aneurysm; a cause of fetal atrial arrhythmias. J Am Coll Cardiol 12:1292–1297
15. Senocak F, Karademir S, Cabuk F, et al. (1996) Spontaneous
closure of interatrial septal openings in infants: an echocardiographic study. Int J Cardiol 53:221–226
16. Shiraishi I, Hamaoka K , Hayashi S, et al. (1990) Atrial septal
aneurysm in infancy. Pediatr Cardiol 11:82–85
17. Silver MD, Dorsey JS (1978) Aneurysms of the septum primum in adults. Arch Pathol Lab Med 102:62–65
18. Snider AR (1997) Defects in cardiac septation. In: Snider
AR, Serwer GA, Ritter SB (eds), Echocardiograpy in Pediatric Heart Disease. Mosby-Year Book, St. Louis, pp 235–
246
19. Timmis GC, Gordon S, Reed JO (1966) Spontaneous physiologic closure of an atrial septal defect. J Am Med Assoc
196:137–139
20. Valenzuela LF, Varquez R, Rodriquez-Hernandez MJ (1999)
Atrial septal aneurysm, is it a benign finding? Int J Cardiol
69:101–103
21. Wolf WJ, Casta AC, Sapire DW (1987) Atrial septal aneurysms in infants and children. Am Heart J 113:1149–1153