Ebook Williams gynecology (Second edition): Part 2
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (41.91 MB, 797 trang )
SECTION 3
FEMALE PELVIC MEDICINE AND
RECONSTRUCTIVE SURGERY
MCGH222-Ch23_605-632.indd 605
05/01/12 1:51 PM
606
CHAPTER 23
Urinary Incontinence
DEFINITIONS .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
EPIDEMIOLOGY .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
RISKS FOR URINARY INCONTINENCE
607
. . . . . . . . . . . . . . . . . . . . . . . . . . .
609
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
609
BLADDER EMPTYING.
. . . . . . . . . . . . . . . . . . . . . . . . . .
CONTINENCE THEORIES .
611
. . . . . . . . . . . . . . . . . . . . . . . .
615
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
616
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
616
DIAGNOSIS .
HISTORY .
607
. . . . . . . . . . . . . .
PATHOPHYSIOLOGY
BLADDER FILLING .
606
PHYSICAL EXAMINATION
. . . . . . . . . . . . . . . . . . . . . . .
618
. . . . . . . . . . . . . . . . . . . . . . . . .
618
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
624
DIAGNOSTIC TESTING .
TREATMENT
CONSERVATIVE/NONSURGICAL.
. . . . . . . . . . . . . . . . . .
TREATMENT OF STRESS URINARY INCONTINENCE .
. . . .
625
. . . . .
628
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
630
TREATMENT OF URGE URINARY INCONTINENCE .
REFERENCES .
624
DEFINITIONS
Urinary incontinence is defined as any involuntary leakage of
urine. In addition to the urethra, urine may also leak from
extraurethral sources, such as fistulas or congenital malformations of the lower urinary tract. Although incontinence is
categorized into a number of forms, this chapter will focus
on the evaluation and management of stress and urge urinary
incontinence. Stress urinary incontinence (SUI) is the involuntary leakage of urine with exertion or with sneezing or coughing. Urge urinary or “urge”—incontinence is the involuntary
leakage accompanied or immediately preceded by a perceived
strong imminent need to void. A related condition, overactive
bladder, describes urinary urgency with or without incontinence and usually with increased daytime urinary frequency
and nocturia (Abrams, 2009).
According to International Continence Society guidelines,
urinary incontinence is a symptom, a sign, and a condition
(Abrams, 2002). For example, with SUI, a patient may complain of involuntary urine leakage with exercise or laughing.
Concurrent with these symptoms, involuntary leakage from the
urethra synchronous with cough or Valsalva may be observed
during examination by a provider. And as a condition, SUI is
objectively demonstrated during urodynamic testing if involuntary leakage of urine is seen with increased abdominal pressure and absence of detrusor muscle contraction. Under these
circumstances, when the symptom or sign of SUI is confirmed
with objective testing, the term urodynamic stress incontinence
(USI), formerly known as genuine stress incontinence, is used.
With urge urinary incontinence, women have difficulty
postponing urination urges and generally must promptly
empty their bladder on cue and without delay. If urge urinary
incontinence is objectively demonstrated during urodynamic
testing with cystometric evaluation, the condition is termed
detrusor overactivity (DO), formerly known as detrusor instability. When both stress and urgency components are present, it
is called mixed urinary incontinence.
Functional incontinence occurs in situations in which a
woman cannot reach a toilet in time because of physical, psychological, or mentation limitations. Often, this group would
be continent if these issues were absent.
Urinary Incontinence
EPIDEMIOLOGY
RISKS FOR URINARY INCONTINENCE
■ Age
The prevalence of incontinence appears to increase gradually
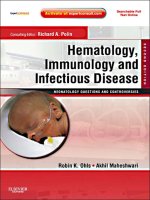
during young adult life (Fig. 23-1). A broad peak is noted at
middle age and then steadily increases after age 65 (Hannestad,
2000). Similarly, data from the 2005-2006 NHANES demonstrate a steady increase in incontinence prevalence with age:
7 percent in those aged 20 to 40 years, 17 percent for ages 40
to 60, 23 percent for ages 60 to 80, and 32 percent for those
older than 80 (Nygaard, 2008).
Incontinence should not be viewed as a normal consequence
of aging. However, several physiologic age-related changes in
the lower urinary tract may predispose to incontinence, overactive bladder, or other voiding difficulties. First, the prevalence of involuntary detrusor contractions increases with age,
and detrusor overactivity is found in 21 percent of healthy,
40
35
Percentage (%)
30
25
20
15
10
5
0
20–24 25–29 30–34 35–39 40–44 45–49 50–54 55–59 60–64 65–69 70–74 75–79 80–84 85+
Unknown
0.3
0.6
1
1.1
1.6
2.4
3
3.1
3.6
4.8
4
4.2
5.2
5.7
Slight
6.3
8
10.7
11.5
11.6
13.7
12.3
9.3
7.8
5.6
5.7
7
5.9
2.6
Moderate
2.5
4.5
4.9
6
7.5
8.3
8.8
8.4
7.6
8.3
8.1
8.1
8.1
8.2
Severe
1.3
1.6
1.6
2.6
3.3
4.1
6.1
6.8
7.2
8.7
12.1
14.6
16.1
19.3
Age (years)
FIGURE 23-1 Prevalence of incontinence by age group (n ϭ 8002). (Adapted from Hannestad, 2000, with permission.)
CHAPTER 23
In Western societies, epidemiologic studies indicate a prevalence
of urinary incontinence of 15 to 55 percent. This wide range
is attributed to variations in research methodologies, population
characteristics, and definitions of incontinence. As part of the
2005-2006 National Health and Nutrition Examination Survey
(NHANES), a cross-sectional group of 1961 nonpregnant, noninstitutionalized women in the United States were questioned
about pelvic floor disorders. Urinary incontinence that was
characterized by participants as moderate to severe leakage was
identified in 15.7 percent (Nygaard, 2008). However, current
available data are limited by the fact that most women do not
seek medical attention for this condition (Hunskaar, 2000). It is
estimated that only one in four women will seek medical advice
for incontinence due to embarrassment, limited access to health
care, or poor screening by health care providers (Hagstad, 1985).
Among ambulatory women with urinary incontinence,
the most common condition is SUI, which represents 29 to
75 percent of cases. Urge urinary incontinence accounts for up
to 33 percent of incontinence cases, whereas the remainder is
attributable to mixed forms (Hunskaar, 2000). In a review of
overactive bladder, 15 percent of 64,528 women met criteria for
overactive bladder with or without incontinence, and 11 percent
had urge urinary incontinence (Hartmann, 2009).
Urinary incontinence can significantly impair a woman’s
quality of life, leading to disrupted social relationships, psychological distress from embarrassment and frustration, hospitalizations due to skin breakdown and urinary tract infection, and
nursing home admission. An incontinent elderly woman is 2.5
times more likely to be admitted to a nursing home than a continent one (Langa, 2002). Likewise, the monetary ramifications of
incontinence are considerable. An estimated $32 billion is spent
annually in the United States caring for community-dwelling
and institutionalized patients with urinary incontinence (Hu,
2004). Moreover, population projections from the U.S. Census
Bureau forecast that the number of American women with urinary incontinence will increase 55 percent from 18.3 million to
28.4 million between 2010 and 2050 (Wu, 2009).
607
608
Female Pelvic Medicine and Reconstructive Surgery
SECTION 3
continent community-dwelling elderly (Resnick, 1995). Total
bladder capacity and the ability to postpone voiding decreases,
and these declines may lead to urinary frequency. In addition,
urinary flow rates are reduced in both older men and women
and likely due to an age-associated decrease in detrusor contractility (Resnick, 1984). In women, postmenopausal decreases
in estrogen levels result in atrophy of the urethral mucosal seal,
loss of compliance, and bladder irritation, which may predispose to both stress and urge urinary incontinence. Finally, there
are age-related changes in renal filtration rate and alterations
in diurnal levels of antidiuretic hormone and atrial natriuretic
factor. These changes shift the diurnal-predominant pattern of
fluid excretion toward one with greater urine excretion later in
the day (Kirkland, 1983).
■ Race
Traditionally, white women are believed to have higher rates of
stress urinary incontinence than women of other races. In contrast, urge urinary incontinence is believed to be more prevalent
among African-American women. Most reports are not population based and thus are not the best estimate of true racial
differences. In addition, existing data on racial differences are
largely based on small sample sizes (Bump, 1993). However,
data from the Nurse’s Health Study cohorts, which included
more than 76,000 women, did support these racial differences.
Investigators found the highest 4-year incidence rates in white
participants compared with that in Asian and black women
(Townsend, 2010). It is not yet clear whether these differences
are biologic, related to health care access, or affected by cultural
expectations and symptom tolerance thresholds.
■ Obesity
Several epidemiologic studies have shown that an increased body
mass index (BMI) is a significant and independent risk factor
for urinary incontinence of all types (Table 23-1). Moreover, the
prevalence of both urge urinary and stress incontinence increases
proportionally with BMI (Hannestad, 2003). Theoretically,
the increase in intraabdominal pressure that coincides with an
TABLE 23-1. Risk Factors for Urinary Incontinence
Age
Pregnancy
Childbirth
Menopause
Hysterectomy
Obesity
Urinary symptoms
Functional impairment
Cognitive impairment
Chronically increased abdominal pressure
Chronic cough
Constipation
Occupational risk
Smoking
increased BMI results in a higher intravesical pressure. This
higher pressure overcomes urethral closing pressure and leads to
incontinence (Bai, 2002). Accordingly, as a greater portion of
our population becomes overweight and obese, we can expect to
see an increase in the prevalence of urinary incontinence in the
United States (Flegal, 2002). Encouragingly, weight loss for many
can be an effective treatment. In overweight or obese women, the
prevalence of urinary incontinence significantly declines following weight loss achieved by behavior modification or with bariatric surgery (Burgio, 2007; Deitel, 1988; Subak, 2009).
■ Menopause
Studies have inconsistently demonstrated an increase in urinary
dysfunction after a woman enters her postmenopausal years
(Bump, 1998). In those with symptoms, separating hypoestrogenism effects from the effects of aging is difficult.
High-affinity estrogen receptors have been identified in
the urethra, pubococcygeal muscle, and bladder trigone but
are infrequently found elsewhere in the bladder (Iosif, 1981).
Hypoestrogenic-related collagen changes and reductions in urethral vascularity and skeletal muscle volume are factors. They
are thought to collectively contribute to impaired urethral function via a decreased resting urethral pressure (Carlile, 1988).
Moreover, estrogen deficiency with resulting urogenital atrophy
is believed to be responsible in part for urinary sensory symptoms following menopause (Raz, 1993). Despite this current
evidence that estrogen plays a role in normal urinary function,
it is less clear whether estrogen therapy is useful in the treatment
or prevention of incontinence (Cody, 2009; Fantl, 1994, 1996).
■ Childbirth and Pregnancy
Many studies reveal the prevalence of urinary incontinence to be
higher in parous women compared with nulliparas. The effects of
childbirth on incontinence may result from direct injury to pelvic muscles and connective tissue attachments. In addition, nerve
damage from trauma or stretch injury may result in pelvic muscle dysfunction. Specifically, rates of prolonged pudendal nerve
latency after delivery are higher in women with incontinence
compared with asymptomatic puerperal women (Snooks, 1986).
One large epidemiologic study identified vaginal delivery
parameters that may affect the risk of urinary incontinence
later in life. First, fetal birthweight Ն4000 g increased the risk
of all urinary incontinence types (Rortveit, 2003b). Secondly,
cesarean delivery may have a short-term protective effect for
preventing urinary incontinence. In this study, the adjusted
odds ratio for any incontinence associated with vaginal delivery
compared with that with cesarean delivery was 1.7 (Rortveit,
2003a). However, the protective effect of cesarean delivery on
incontinence may dissipate after additional deliveries, decreases
with age, and is not present in older women (Nygaard, 2006).
■ Family History
Evidence suggests that the risk of urinary incontinence may be
increased in the daughters and sisters of incontinent women.
In one large survey, daughters of incontinent women had an
increased relative risk of 1.3 and absolute risk of 23 percent
Urinary Incontinence
of having urinary incontinence. Younger sisters of incontinent
women also had a greater likelihood of having any urinary
incontinence (Hannestad, 2004).
In women older than 60 years with chronic obstructive pulmonary disease, a significantly increased risk of urinary incontinence is found (Brown, 1996; Diokno, 1990). Similarly,
cigarette smoking is identified as an independent risk factor for
urinary incontinence in several studies. Both current and former
smokers were noted to have a two- to threefold risk of incontinence compared with nonsmokers (Brown, 1996; Bump, 1992;
Diokno, 1990). In another study, investigators also identified
an association between current and former smoking and incontinence, but only for those who smoked more than 20 cigarettes
daily. Severe incontinence was weakly associated with smoking
regardless of cigarette number (Hannestad, 2003). Theoretically,
persistently increased intraabdominal pressures are generated
from a smoker’s chronic cough, and collagen synthesis is diminished by smoking’s antiestrogenic effects.
■ Hysterectomy
Studies have inconsistently shown that hysterectomy is a risk
factor for developing urinary incontinence. Those that show an
association are retrospective, lack appropriate control groups,
and are often based solely on subjective data (Bump, 1998).
In contrast, studies that include pre- and postoperative urodynamic testing reveal clinically insignificant changes in bladder
function. Moreover, evidence does not support avoidance of
clinically indicated hysterectomy or the selection of supracervical hysterectomy as measures to prevent urinary incontinence
(Vervest, 1989; Wake, 1980).
PATHOPHYSIOLOGY
■ Continence
The bladder is a urine storage organ with the capacity to accommodate large increases in volume with minimal or no increases in
intravesical pressure. The ability to store urine coupled with convenient and socially acceptable voluntary emptying is continence.
Continence requires the complex coordination of multiple
components that include: muscle contraction and relaxation,
appropriate connective tissue support, and integrated innervation and communication between these structures. Simplistically,
during filling, urethral contraction is coordinated with bladder relaxation and urine is stored. During voiding, the urethra
relaxes and the bladder contracts. These mechanisms can be challenged by uninhibited detrusor contractions, marked increases
in intraabdominal pressure, and changes to the various anatomic
components of the continence mechanism.
■ Bladder Filling
Bladder Anatomy
The bladder wall is multilayered and contains mucosal, submucosal, muscular, and adventitial layers (Fig. 23-2). The bladder
Innervation Overview
Normal function of the lower urinary tract requires integration of peripheral and central nervous systems. The peripheral
nervous system contains somatic and autonomic divisions (Fig.
23-3). Of these, the somatic component innervates striated muscle, whereas the autonomic division innervates smooth muscle.
The autonomic nervous system controls involuntary motion
and is categorized into sympathetic and parasympathetic divisions. The sympathetic system mediates its end-organ effects
through epinephrine or norepinephrine acting on ␣- or
-adrenergic receptors (Fig. 23-4). The parasympathetic division acts through acetylcholine binding to muscarinic or nicotinic receptors. In the pelvis, autonomic fibers that supply the
pelvic viscera course in the superior and inferior hypogastric
plexi (Fig. 23-5).
The somatic nervous system controls voluntary movement,
and the portion of this system that is most relevant to lower
urinary tract function originates from Onuf somatic nucleus
(p. 613). This nucleus is located in the ventral horn gray matter of spinal levels S2–S4 and contains the neurons that innervate the striated urogenital sphincter complex, described next.
Nerves involved with that connection include branches of the
pudendal and pelvic nerves.
Urogenital Sphincter
As the bladder fills, synchronized contraction of the urogenital
sphincter is integral to continence. Composed of striated muscle, this sphincter complex includes: (1) the sphincter urethrae,
(2) the urethrovaginal sphincter, and (3) the compressor urethrae.
The sphincter urethrae wraps circumferentially around the urethra. In comparison, the urethrovaginal sphincter and the compressor urethrae arch ventrally over the urethra and insert into
the fibromuscular tissue of the anterior vaginal wall (Fig. 23-6).
These three muscles function as a single unit and contract to
close the urethra. Contraction of these muscles circumferentially
constricts the cephalad two thirds of the urethra and laterally
compresses the distal one third. The sphincter urethrae is predominantly composed of slow-twitch fibers and remains tonically contracted, contributing substantially to continence at rest.
In contrast, the urethrovaginal sphincter and the compressor
CHAPTER 23
■ Smoking and Chronic Lung Disease
mucosa is comprised of a transitional cell epithelium, supported
by a lamina propria. With small bladder volumes, the mucosa is
thrown into convoluted folds. However, with bladder filling, it
is stretched and thinned. The bladder epithelium, termed uroepithelium, is comprised of distinct cell layers. The most superficial is the umbrella cell layer, and its impermeability is thought
to provide the primary urine-plasma barrier. Covering the
uroepithelium is a glycosaminoglycan (GAG) layer. This GAG
layer may prohibit bacterial adherence and prevents urothelial
damage by acting as a protective barrier. Specifically, theories
suggest that this carbohydrate polymer layer may be defective
in patients with interstitial cystitis (Chap. 11, p. 320).
The muscular layer, termed the detrusor muscle, is composed of three smooth-muscle layers arranged in a plexiform
fashion. This unique arrangement allows for rapid multidimensional expansion during bladder filling and is a key component
to the bladder’s ability to accommodate large volumes.
609
610
Female Pelvic Medicine and Reconstructive Surgery
Median umbilical
ligament
SECTION 3
Ureter
Peritoneum
Detrusor muscle
Ureteral openings
Trigone
Neck of urinary bladder
Transitional
epithelium
Mucosa
Lamina propria
Submucosa
Internal urethral
sphincter
Detrusor muscle
Urogenital sphincter in
the perineal membrane
Adventitia
A
Transitional epithelium
Lamina propria
LM 78x
Transitional
epithelium
Lamina propria
Submucosa
Detrusor muscle
of muscularis
LM 18x
B
urethrae are comprised of fast-twitch muscle fibers, which allow
brisk contraction and urethra lumen closure when continence
is challenged by sudden increases in intraabdominal pressure.
Innervation Important to Storage
The urogenital sphincter receives somatic motor innervation
through the pudendal and pelvic nerves (see Figs. 23-5 and 23-7).
FIGURE 23-2 Bladder anatomy. A. Anteroposterior
view of bladder anatomy. Inset: The bladder wall
contains mucosal, submucosal, muscular, and
adventitial layers. B. Photomicrograph of the
bladder wall. The mucosa of an empty bladder is
thrown into convoluted folds or rugae. The plexiform arrangement of muscle fibers of the detrusor
muscle cause difficulty in defining its three distinct
layers. (From McKinley, 2006, with permission.)
Thus, pudendal neuropathy, which may follow obstetric injury,
can affect normal sphincter functioning. Additionally, prior
pelvic surgery or pelvic radiation therapy may damage nerves,
vasculature, and soft tissue. Such injury can lead to ineffective
urogenital sphincter action and contribute to incontinence.
Sympathetic fibers are carried through the superior hypogastric nerve plexus and communicate with ␣- and -adrenergic
Urinary Incontinence
Central
nervous system
Peripheral
nervous system
Somatic nervous
system
Smooth muscle
Striated muscle
Sympathetic division
Parasympathetic division
α-adrenergic receptors
β-adrenergic receptors
Muscarinic receptors
Nicotinic receptors
FIGURE 23-3 Divisions of the human nervous system. The
peripheral nervous system includes: (1) the somatic nervous system, which mediates voluntary movements through its actions
on striated muscle, and (2) the autonomic nervous system, which
controls involuntary motion through its actions on smooth muscle.
The autonomic nervous system is further divided into the sympathetic division, which acts through epinephrine and norepinephrine binding to adrenergic receptors, and the parasympathetic
division, which acts through acetylcholine binding to muscarinic
or nicotinic receptors.
receptors within the bladder and urethra. -Adrenergic receptor stimulation in the bladder dome results in smooth-muscle
relaxation and assists with urine storage (Fig. 23-8). In contrast, ␣-adrenergic receptors predominate in the bladder base
and urethra. These receptors are stimulated by norepinephrine,
which initiates a cascade of events that preferentially leads to
urethral contraction and aids urine storage and continence.
These effects of ␣-stimulation underlie the treatment of SUI
with imipramine, a tricyclic antidepressant with adrenergic
agonist properties.
Urethral Coaptation
One key to maintaining continence is adequate urethral mucosal
coaptation. The uroepithelium is supported by a connective tissue layer, which is thrown into deep folds, also known as plications. A rich capillary network runs within its subepithelial layer.
This vascular network aids in urethral mucosal approximation,
also termed coaptation, by acting like an “inflatable cushion”
(Fig. 23-9). In women who are hypoestrogenic, this submucosal
vasculature plexus is less prominent. In part, hormone replacement targets this diminished vascularity and enhances coaptation
to improve continence.
■ Bladder Emptying
Innervation Related to Voiding
When an appropriate time for bladder emptying arises, sympathetic stimulation is reduced and parasympathetic stimulation
is triggered. Specifically, neural impulses carried in the pelvic
nerves stimulate acetylcholine release and lead to detrusor
muscle contraction (Fig. 23-10). Concurrent with detrusor
stimulation, acetylcholine also stimulates muscarinic receptors
in the urethra and leads to outlet relaxation for voiding.
Within the parasympathetic division, acetylcholine receptors are broadly defined as muscarinic and nicotinic. The
bladder is densely supplied with muscarinic receptors, which
FIGURE 23-4 The bladder dome is rich in parasympathetic muscarinic receptors (M) and sympathetic -adrenergic receptors (). The
bladder neck contains a greater density of sympathetic ␣-adrenergic receptors (␣).
CHAPTER 23
Autonomic nervous
system (ANS)
611
612
Female Pelvic Medicine and Reconstructive Surgery
SECTION 3
FIGURE 23-5 The inferior hypogastric plexus, also known as the pelvic plexus, is formed by visceral efferents from S2 to S4, which provide the parasympathetic component by way of the pelvic nerves. The superior hypogastric plexus primarily contains sympathetic fibers
from the T10 to L2 cord segments and terminates by dividing into right and left hypogastric nerves. The hypogastric nerves and rami
from the sacral portion of the sympathetic chain contribute the sympathetic component to the pelvic plexus. The pelvic plexus divides
into three portions according to the course and distribution of its fibers: the middle rectal plexus, uterovaginal plexus, and vesical plexus.
Muscular Activity with Voiding
is ideally suited for rapid concentric contraction during bladder
emptying.
During voiding, all components of the striated urogenital sphincter relax. Importantly, bladder contraction and
sphincter relaxation must be coordinated for effective voiding.
Occasionally, in a condition known as detrusor sphincter dyssynergia, the urethral sphincter fails to relax during contraction of
the detrusor, and retention ensues. Women with this condition
may be treated with pharmacologic agents such as muscle relaxants. These drugs purportedly relax the urethral sphincter and
levator ani muscles to improve coordinated voiding.
Smooth muscle cells within the detrusor fuse with one another
so that low-resistance electrical pathways extend from one muscle cell to the next. Thus, action potentials can spread quickly
throughout the detrusor muscle to cause rapid contraction of
the entire bladder. In addition, the plexiform arrangement of
bladder detrusor fibers allows multidirectional contraction and
Theories on continence abound and vary in their supporting scientific evidence. Most theories can ultimately be distilled down
to those that involve the concepts of anatomic stress incontinence and decreased urethral integrity (sphincteric deficiency).
when stimulated lead to detrusor contraction. Of the muscarinic receptors, five glycoproteins designated M1–M5 have been
identified. M2 and M3 receptor subtypes have been identified as
the ones predominantly responsible for detrusor smooth muscle contraction. Thus, treatment with muscarinic antagonist
medication blunts detrusor contraction to improve continence.
Specifically, continence drugs that target only the M3 receptor
maximize drug efficacy yet minimize activation of other muscarinic receptors and drug side effects.
■ Continence Theories
FIGURE 23-6 Striated urogenital sphincter anatomy. The perineal membrane is removed to show the three component muscles of the
striated urogenital sphincter. This sphincter receives most of its somatic innervation through the pudendal nerve.
FIGURE 23-7 Onuf nucleus is found in the ventral horn gray matter of S2 through S4. This nucleus contains the neurons whose fibers
supply the striated urogenital sphincter. The urethrovaginal sphincter and compressor urethrae are innervated by the perineal branch of
the pudendal nerve. The sphincter urethrae is variably innervated by somatic efferents that travel in the pelvic nerves.
614
Female Pelvic Medicine and Reconstructive Surgery
SECTION 3
FIGURE 23-8 Physiology of urine storage. Bladder distension from filling leads to: (1) ␣-adrenergic contraction of the urethral smooth
muscle and increased tone at the vesical neck (via the T11-L2 spinal sympathetic reflex); (2) activation of urethral motor neurons in Onuf
nucleus with contraction of striated urogenital sphincter muscles (via the pudendal nerve); and (3) inhibited parasympathetic transmission
with decreased detrusor pressure. ␣ ϭ alpha adrenergic receptors;  ϭ beta adrenergic; M ϭ muscarinic (cholinergic).
A
B
FIGURE 23-9 Drawing of urethral anatomy. A. Urethral anatomy in cross section. Urethral coaptation results in part from filling of the rich
subepithelial vascular plexus. The urethra contains circular and longitudinal smooth muscle layers. B. Vesical neck and urethral anatomy.
The striated urogenital sphincter lies external to the urethral smooth muscle layers.
Urinary Incontinence
615
CHAPTER 23
FIGURE 23-10 Physiology of urine evacuation. Efferent impulses from the pontine micturition center results in inhibition of somatic
fibers in Onuf nucleus and voluntary relaxation of the striated urogenital sphincter muscles. These efferent impulses also result in
preganglionic sympathetic inhibition with opening of the vesical neck and parasympathetic stimulation, which results in detrusor
muscarinic contraction. The net result is relaxation of the striated urogenital sphincter complex causing decreased urethral pressure,
followed almost immediately by detrusor contraction and voiding. ␣ ϭ alpha adrenergic receptors;  ϭ beta adrenergic; M ϭ
muscarinic (cholinergic).
Anatomic Stress Incontinence
Urethral and bladder neck support is integral to continence.
This support stems from: (1) ligaments along the urethra’s lateral aspects, termed the pubourethral ligaments; (2) the vagina
and its lateral fascial condensation; (3) the arcus tendineus fascia pelvis; and (4) levator ani muscles. A full anatomic description of these ligaments and muscles is found in Chapter 38
(p. 925).
In an ideally supported urogenital tract, increases in intraabdominal pressure are equally transmitted to the bladder, bladder base, and urethra. In women who are continent, increases
in downward-directed pressure from cough, laugh, sneeze, and
Valsalva maneuver are countered by supportive tissue tone provided by the levator ani muscles and vaginal connective tissue
(Fig. 23-11). With loss of support, the ability of the urethra and
bladder neck to close against a firm supportive “backboard” is
Abdominal
cavity
Abdominal
cavity
Valsalva
Bladder
Symphysis
Bladder
Urethra
Urethra
FIGURE 23-11 Drawing describes the pressure transmission
theory. In women with normal support (left image), increases in
intraabdominal pressure are equally distributed to contralateral
sides of the bladder and urethra. In those with poor urethral support (right image), increases in intraabdominal pressure alter the
urethrovesical angle, and continence may be lost.
616
Female Pelvic Medicine and Reconstructive Surgery
SECTION 3
diminished. This results in reduced urethral closing pressures,
an inability to resist increases in bladder pressure, and in turn,
incontinence. This mechanistic theory is the basis for surgical
reestablishment of this support. Procedures such as Burch and
Marshall-Marchetti-Kranz (MMK) colposuspensions attempt
to return this anatomic support to the urethrovesical junction
and proximal urethra.
Sphincteric Deficiency
Factors Affecting Urethral Integrity. The urethra maintains continence through the combination of urethral mucosal coaptation, the underlying urethral vascular plexus, the
combined viscous and elastic properties of the urethral epithelium, and contraction of appropriate surrounding musculature. Defects in any of these components may lead to
urine leakage. For example, prior surgery in the retropubic
space may cause denervation and scarring of the urethra and
its supporting tissue. These effects subsequently prevent urethral closure and lead to incontinence. This urethral state
is termed intrinsic sphincteric defect (ISD) and colloquially
is referred to as a “lead pipe” urethra. With ISD, denervation and/or devascularization of the urethra are common
underlying findings. Specific causes are varied and include
prior pelvic reconstructive surgeries, prior pelvic radiation
therapy, diabetic neuropathy, neuronal degenerative diseases,
and hypoestrogenism. In women with atrophic lower genital
tracts, vascular changes within the plexus surrounding the
urethra lead to poor coaptation and greater risks of incontinence.
As noted earlier, nerve dysfunction following birth trauma
may lead to defective urethral sphincter function. In addition,
childbirth also commonly injures urethral fascial support. This
clinical example highlights the intimate relationship between
urethral support and integrity.
Restoration of Urethral Integrity. Treatments to restore
urethral integrity include transurethral injection of bulking agents, surgical sling procedures, and pelvic floor muscle
strengthening and are described in later sections of this chapter. In brief, bulking agents are placed at the urethrovesical
junction to elevate the epithelium and promote coaptation.
Alternatively, the partial urethral obstruction created by pubovaginal sling procedures enhances urethral integrity. Lastly,
because the urethra exits through urogenital hiatus, conditioning of the levator ani muscles with Kegel exercises can bolster
urethral integrity. These muscles can be contracted around the
urethra when continence is challenged by sudden increases in
intraabdominal pressures.
DIAGNOSIS
■ History
Symptom Clustering
To quantify symptoms, investigators have created various validated patient questionnaires (Kelleher, 1997; Patrick, 1999;
Wagner, 1996). Many of these are lengthy and may be impractical for general clinical practice. More simply, assessment of
incontinence begins with a patient describing her urinary symptoms. This inventory of complaints may be collected through
direct conversation but can be augmented with a patient questionnaire as shown in Table 23-2.
During inquiry, the number of voids and pads used per day,
type of pad, frequency of pad changing, and the degree of pad
TABLE 23-2. Review of Systems for Women with Urinary Incontinence
Leak with stress
Y/N
Leak with urge
Y/N
Leak with position changes
Y/N
Leak with exercise
Y/N
Leak with intercourse/orgasm
Y/N
Unconscious leakage
Y/N
Duration of symptoms _____ week(s) _____ month(s)
_____ year(s)
Leaks per _____ day _____ week(s) _____ month(s)
Pads per day _____ Type of pads _____
Voids daytime: _____
Voids nighttime: _____
Constipation Y/N
Self-medicate with ____________________
BMs _____/day _____/week
Anal incontinence
Y/N
Duration _____ month(s) _____ year(s)
Flatus _____/week(s) _____/month(s)
Liquid _____/week(s) _____/month(s)
Stool
_____/week(s) _____/month(s)
BM ϭ bowel movement; UTI ϭ urinary tract infection.
Digital decompression of bowel
Digital decompression of bladder
Postvoid dribble
Feeling of incomplete emptying
Recurrent UTI __________/yr
Void with Valsalva
Urine stream: strong/normal/weak
Childhood enuresis
Frequency
Urgency
Dysuria
Hematuria
Back pain
Pelvic pressure/Bulge
Dyspareunia
Rectal bleeding
Does heavy lifting
Interferes w/lifestyle or quality of life
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Y/N
Urinary Incontinence
TABLE 23-3. Symptom Comparison of Women with
Stress or Urge Incontinence
Symptom
Urge
Incontinence
Stress
Incontinence
Urgency
Yes
No
Frequency with
urgency
Yes
No
Urine leakage
with increased
intraabdominal
pressures
No
Yes
Amount of urinary
leakage with
each incontinence
episode
Large
Small
Ability to reach the
toilet in time
following an urge
to void
Often no
Yes
Waking to void at
night
Usually
Seldom
Bladder Diary
Please record the time and amount of your oral intake, urine output,
urine leakage, and pad changes FOR 3 DAYS
Time
Oral Intake
Voided Urine
Urine Leakage
or Pad Change
FIGURE 23-12 Example of an abbreviated urinary diary.
Voiding Diary
Typically, patients may not have an entirely accurate recollection of their own voiding habits. Accordingly, to obtain a
thorough record, a woman should complete a urinary diary
(Fig. 23-12). With this, women are instructed to record for
3 to 7 days the volumes and type of each oral fluid intake,
volumes of urine with each void, episodes of urinary leakage, and provokers of incontinence episodes. During each
24-hour period, women should also record times of sleep
and awakening. This enables an accurate description of
voluntary nocturnal voiding patterns as well as enuresis.
Although 5 to 7 days of documentation is desirable, 3 days
will suffice in determining the general trend of incontinence.
Realistically, most patients are typically not compliant for
more than 3 days.
The historical information gained from a voiding/urinary
diary is a valuable diagnostic and sometimes therapeutic tool.
The first morning void is usually the largest of the day and is a
good estimate of bladder capacity. Patients often can identify
patterns in intake and voiding and modify behavior. For example, a patient may recognize increased urinary frequency or urge
urinary incontinence episodes after caffeine intake. Moreover,
this diary information serves as a baseline against which treatment efficacy can be assessed.
Urinary Symptoms
Urinary Frequency. Most women void eight times per day
or less. Without a history that reflects increased fluid intake,
increased voiding may indicate overactive bladder, urinary
tract infection (UTI), calculi, or urethral pathology and should
prompt additional evaluation. In addition, urinary frequency is
commonly associated with interstitial cystitis (IC). In women
with IC, the numbers of voids may commonly exceed 20 per
day. In women with urge urinary incontinence or in those
with systemic fluid management disorders such as congestive
heart failure, nocturia may be noted. In the latter case, treatment of the underlying condition frequently leads to symptom
improvement or cure of nighttime frequency.
Urinary Retention. It is important to determine if the
patient adequately empties her bladder. Often incomplete emptying can result in incontinence associated with either stress or
CHAPTER 23
saturation are important considerations. Although these specifics alone may not establish the exact type of incontinence, it
does provide information regarding symptom severity and its
effects on patient activities. Obviously, if a woman’s symptoms
do not diminish her quality of life, then simple observation is
reasonable. Conversely, those with disruptive symptoms warrant further evaluation.
Specific to incontinence, information that describes the
circumstances in which leakage occurs and specific maneuvers
that incite or provoke leakage should be sought. With SUI,
provokers may include increases in intraabdominal pressure
such as coughing, sneezing, Valsalva maneuver, or thrusting
during intercourse (Table 23-3). Alternatively, women with
urge urinary incontinence may describe a loss of urine after
urge sensations that typically cannot be suppressed. Overflow
incontinence was a term used in the past to refer to women
who had an inability to empty their bladder and had episodes
of incontinence associated with urgency. Currently, however,
this is considered by most to reflect another presentation of
urge urinary incontinence. These women often note a sudden
large loss of urine that is preceded by an inability to empty
their bladder.
During questioning, symptoms typically cluster into those
most frequently seen with SUI or with urge urinary incontinence. Alternatively, a significant overlap of complaints may
reflect coexistent SUI and urge urinary incontinence, that is,
mixed urinary incontinence. For these reasons, pattern identification is helpful as it may direct diagnostic testing and guide
initial empiric therapy.
617
618
Female Pelvic Medicine and Reconstructive Surgery
urgency. As described earlier, the term overflow incontinence is
no longer used.
SECTION 3
Other Urinary Symptoms. The volume of urine lost with
each episode may also provide diagnostic clues. Large volumes
are typically lost following a spontaneous detrusor contraction associated with urge urinary incontinence and may often
involve loss of the entire bladder volume. In contrast, woman
with SUI usually describe smaller volumes lost. Moreover, these
women often are able to contract the levator ani muscles to
temporarily stop their urine stream.
Postvoid dribbling is classically associated with urethral
diverticulum, which may often be mistaken for urinary incontinence (Chap. 26, p. 683). Hematuria, although a common
sign of UTI, may also indicate underlying malignancy and can
cause irritative voiding symptoms.
The onset of symptoms may also provide information
regarding etiology and treatment. For example, onset of symptoms with the menopause may suggest hypoestrogenism as an
etiology. These patients may benefit from topical vaginal estrogen. In contrast, symptoms after hysterectomy or childbirth
may reflect changes in tissue support or innervation.
Past Medical History
Obstetric trauma may be associated with damage to pelvic floor support, which may lead to SUI. For this reason,
information describing a prolonged labor, operative vaginal
delivery, macrosomia, postpartum catheterization for urinary
retention, and increased parity may be valuable. As alluded
to earlier, urinary incontinence may be associated with several medical conditions or their treatments, which could be
modified to improve incontinence. To help remember these
potential contributors, a useful mnemonic is “DIAPPERS”:
dementia/delirium, infection, atrophic vaginitis, psychological, pharmacologic, endocrine, restricted mobility, and stool
impaction (Swift, 2008).
First, continence requires the cognitive ability to recognize
and react appropriately to the sensation of a full bladder, motivation to maintain dryness, sufficient mobility and manual
dexterity, and ready access to a toilet. Patients with dementia
or significant psychological impairments often do not have the
necessary cognitive ability for continence maintenance. Women
with severe physical handicaps or restricted mobility may simply not have time to reach the toilet, especially in the setting of
urinary urgency/overactive bladder.
Urinary tract infections cause bladder mucosal inflammation. This inflammation is thought to increase sensory afferent
activity, which contributes to an overactive bladder. Similarly,
estrogen deficiency may lead to atrophic vaginitis and urethritis. These are associated with increased local irritation and
greater risks of UTI and overactive bladder.
A detailed medication inventory should be collected. Pertinent
drugs may include estrogen, ␣-adrenergic agonists, and diuretics
(Table 23-4).
Diabetes mellitus can lead to osmotic diuresis and polyuria
if glucose control is poor. Polydipsia from diabetes insipidus
or excessive caffeine or alcohol intake can also lead to polyuria
or urinary frequency. Similarly, other disorders of impaired
arginine vasopressin secretion or action may cause polyuria
and nocturia (Ouslander, 2004). Conditions such as congestive heart failure, hypothyroidism, venous insufficiency, and
the effects of certain medications all contribute to peripheral
edema, leading to urinary frequency and nocturia when a
patient is supine.
Finally, stool impaction resulting from poor bowel habits
and constipation can contribute to overactive bladder symptoms. This is perhaps from local irritation or direct compression
against the bladder wall.
■ Physical Examination
General Inspection and Neurologic Evaluation
Initially, the perineum is inspected for evidence of atrophy,
which may be noted throughout the lower genital tract. In addition, suburethral bulging with transurethral expression of fluid
during forward-directed compression suggests a urethral diverticulum (Fig. 26-3, p. 683).
A thorough physical examination for a woman with incontinence should also include a detailed neurologic evaluation
of the perineum. Because neurologic responses may be altered
in an anxious patient who is in a vulnerable setting, signs
elicited during examination may not signify true pathology
and should be interpreted with caution. Neurologic evaluation begins with an attempt to elicit a bulbocavernosus reflex.
During this test, one labium majora is stroked with a cotton swab. Normally, both labia equally contract bilaterally. The afferent limb of this reflex is the clitoral branch of
the pudendal nerve, whereas its efferent limb is conducted
through the inferior hemorrhoidal branch of the pudendal
nerve. This reflex is integrated at the S2-S4 spinal cord level
(Wester, 2003). Thus, reflex absence may reflect central or
peripheral neurologic deficits. Secondly, a normal circumferential anal sphincter contraction, colloquially called an “anal
wink,” should follow cotton swab brushing of the perianal
skin. External urethral sphincter activity requires at least
some degree of intact S2-S4 innervation, and this anocutaneous reflex is mediated by the same spinal neurologic level.
Thus, an absent wink may indicate deficits in this neurologic
distribution.
Pelvic Support Assessment
Pelvic Organ Prolapse Evaluation. Poor urethral support
commonly accompanies pelvic organ prolapse (POP). For
example, women with significant prolapse are often unable to
completely empty their bladder due to urethral kinking and
obstruction. These women frequently must digitally elevate or
reduce their prolapse to allow emptying. Thus, an external evaluation for POP, as described in Chapter 24 (p. 644) is indicated
for all women with urinary incontinence. Following this evaluation for vaginal compartment defects, pelvic muscle strength
should also be assessed. Women with mild to moderate urinary
incontinence often respond well to pelvic floor therapy, and
under these circumstances, a trial of this therapy is warranted
and often curative (p. 624).
Urinary Incontinence
619
TABLE 23-4. Medications That May Contribute to Incontinence
Examples
Mechanism
Effect
Alcohol
Beer, wine, liquor
Diuretic effect, sedation,
immobility
Polyuria, frequency
␣-Adrenergic agonists
Decongestants, diet pills
IUS contraction
Urinary retention
␣-Adrenergic blockers
Prazosin, terazosin, doxazosin
IUS relaxation
Urinary leakage
Inhibit bladder contraction,
sedation, fecal impaction
Urinary retention
and/or functional
incontinence
Anticholinergic
agents
Antihistamines
Antipsychotics
Antiparkinsonians
Miscellaneous
Skeletal muscle
relaxants
Tricyclic
antidepressants
Diphenhydramine, scopolamine,
dimenhydrinate
Thioridazine, chlorpromazine,
haloperidol
Trihexyphenidyl, benztropine
mesylate
Dicyclomine, disopyramide
Orphenadrine, cyclobenzaprine
Amitriptyline, imipramine,
nortriptyline, doxepin
ACE inhibitors
Enalapril, captopril, lisinopril, losartan
Chronic cough
Urinary leakage
Calcium-channel
blockers
Nifedipine, nicardipine, isradipine,
felodipine
Relaxes bladder, fluid
retention
Urinary retention,
nocturnal diuresis
COX-2 inhibitors
Celecoxib
Fluid retention
Nocturnal diuresis
Diuretics
Caffeine, HCTZ, furosemide,
bumetanide, acetazolamide,
spironolactone
Increases urinary frequency,
urgency
Polyuria
Narcotic analgesics
Opiates
Relaxes bladder, fecal
impaction, sedation
Urinary retention,
and/or functional
incontinence
Thiazolidinediones
Rosiglitazone, pioglitazone,
troglitazone
Fluid retention
Nocturnal diuresis
ACE ϭ angiotensin-converting enzyme; COX-2 ϭ cyclooxygenase-2; HCTZ ϭ hydrochlorothiazide; IUS ϭ internal urethral
sphincter; NSAID ϭ nonsteroidal antiinflammatory drug.
Q-tip Test. If a urethra is poorly supported, it may display
hypermobility during increases in intraabdominal pressures. To
assess mobility, a clinician places the soft end of a cotton swab
into the urethra to the urethrovesical junction. Failure to insert
the swab to this depth typically leads to errors in assessment
of urethrovesical junction support. Termed the Q-tip test, this
evaluation may be uncomfortable, and application of intraurethral analgesia may prove helpful. Commonly, 1-percent
lidocaine jelly is placed on the cotton swab prior to insertion.
Following placement, a Valsalva maneuver is prompted, and the
swab-excursion angle at rest and with Valsalva maneuver is measured with a goniometer or standard protractor (Fig. 23-13).
An excursion angle from rest and with Valsalva maneuver that
measures Ͼ30 degrees above the horizontal plane indicates urethral hypermobility. The utility of this test is controversial given
that many asymptomatic women with urethral hypermobility
do not have urinary incontinence.
Bimanual and Rectovaginal Examination
In general, these portions of the pelvic examination provide fewer
diagnostic clues to underlying incontinence causes. However,
bimanual examination may reveal an enlarged pelvic mass or a
uterus enlarged by leiomyomas or adenomyosis. These may create incontinence through increased external pressure transmitted
to the bladder. In addition, stool impaction is easily identified
with rectal examination.
CHAPTER 23
Medication
620
Female Pelvic Medicine and Reconstructive Surgery
SECTION 3
A
B
FIGURE 23-13 Drawing depicting Q-tip test in a patient with urethral hypermobility. A. Angle of the Q-tip at rest. B. Angle of the Q-tip
with Valsalva maneuver or other increases in intraabdominal pressure. The urethrovesical junction descends, causing upward deflection
of the Q-tip.
■ Diagnostic Testing
Urinalysis and Culture
In all women with urinary incontinence, infection or urinary
tract pathology must be excluded. Urinalysis and urine culture
are sent at an initial visit, and infection is treated as described in
Table 3-24 (p. 94). Persistent symptoms typically warrant additional evaluation for stress and urge urinary incontinence or for
other conditions such as interstitial cystitis.
of removing the urinary catheter, then a catheter is replaced, and
the test is repeated a day or more later.
During an active bladder trial, the bladder is actively filled with
a set volume, and following patient voiding, residual bladder urine
volumes are calculated. Initially, the bladder is completely emptied by catheterization. It may be helpful during catheterization
for a woman to stand upright to clear the most dependent portions of her bladder. Sterile water is infused under gravity into the
Postvoid Residual (PVR)
This volume is routinely measured during incontinence evaluation. After a woman voids, the PVR may be measured with
a handheld sonographic bladder scanner or by transurethral
catheterization. Portable three-dimensional ultrasound devices
are used to scan the bladder and provide numerical results (Fig.
23-14). In general, they are quick, easy to use, and more comfortable for the patient. However, if using a handheld scanner,
care must be taken in women with an enlarged leiomyomatous uterus as this may falsely record a large PVR. In these
instances, or if a scanner is not available, transurethral catheterization may be used to confirm residual bladder volume.
A large postvoid residual may often reflect one of several
problems including recurrent infection, urethral obstruction
from a pelvic mass, or neurologic deficits. In contrast, a normally small PVR is often found in those with SUI.
Postoperative Postvoid Residual. After antiincontinence
surgery, PVR measurement is a helpful indicator of a patient’s
ability to completely empty her bladder. This evaluation may be
completed with a “passive” or an “active” voiding trial.
With a passive trial, a urinary catheter is removed, and the
PVR is measured by scanner or by transurethral catheterization
after each voluntary void on two occasions. A voided volume
of at least 300 mL and PVR less than 100 mL is desirable.
However, adequate bladder emptying is assumed if the PVR is
less than one third of the voided volume. If the patient does not
meet these criteria, or if she is unable to void within 4 to 6 hours
FIGURE 23-14 Handheld bladder scanner aids estimation of
bladder volume. (Photograph courtesy of Dr. Heather Gardow.)
Urinary Incontinence
Urodynamic Studies
Surgical correction of incontinence is invasive and not without risk. However, the “bladder is an unreliable witness,” and
historical information may not always accurately indicate the
true underlying type of incontinence (Blaivas, 1996). Thus,
if initial conservative management is unsuccessful or surgical
treatment is anticipated, then objective assessment should be
pursued. In addition, if symptoms and physical findings are
incongruous, then objective urodynamic studies (UDS), using
simple or multichannel cystometrics, may also be indicated.
For example, in women with mixed urinary incontinence, who
have symptoms of both stress and urge urinary incontinence,
UDS may reveal that only the urge component is responsible
for their incontinence. Most of these women are treated with
behavioral, physical, and/or pharmacologic therapy initially.
Thus, if identified by UDS, these individuals can avoid unnecessary surgery. Additionally, surgical therapy may be modified
if UDS reveals parameters consistent with intrinsic sphincteric
defect.
Despite these indications, UDS remains controversial.
Leakage noted during testing is not always clinically relevant. In addition, testing may be uninformative if the original offending maneuver or situation that led to incontinence
cannot be reproduced during evaluation. Moreover, objective
confirmation of the diagnosis is not always necessary, since
empiric nonsurgical therapy in women with urge predominant
symptoms is reasonable.
Simple Cystometrics. Objective measurements of bladder
function are combined in a battery of tests termed cystometrics,
which may be simple or multichannel. Simple cystometrics allows
determination of stress incontinence and detrusor overactivity as
well as measurement of first sensation, desire to void, and bladder
capacity. This procedure is easily performed with room-temperature sterile normal saline, 60-mL catheter-tipped syringe, and
urinary catheter, either Foley or Robnell. The urethra is sterilely
prepared, the catheter is inserted, and the bladder is drained. A
60-mL syringe with its plunger removed is attached to the catheter and is filled upright with sterile water. Water is added in
increments until a woman feels a sensation of bladder filling,
urge to void, and bladder maximum capacity. A normal bladder capacity for most women will range from 300 to 700 mL.
Changes in the fluid meniscus within the syringe are monitored.
In the absence of a cough or Valsalva maneuver that would raise
intraabdominal pressure, an abrupt meniscus elevation indicates
bladder contraction and suggests a diagnosis of detrusor overactivity. Once bladder capacity is reached, the catheter is removed,
and the woman is asked to perform a Valsalva maneuver or
cough while standing. Leakage directly linked to these increases
in intraabdominal pressure indicates SUI.
Simple cystometrics are easy to perform, require inexpensive
equipment, and can typically be completed by most gynecologists. One limitation of simple cystometric testing, however, is
its inability to assess for intrinsic sphincteric deficiency (ISD),
which may preclude certain surgical options. Multichannel cystometrics can evaluate for ISD and thus may offer advantages.
Multichannel Cystometrics. This objective urodynamic
study provides more information on other physiologic bladder parameters that are not afforded by simple cystometrics.
Multichannel cystometrics more commonly is performed by
urogynecologists or urologists due to the expense and limited
availability of the equipment. Testing can be performed with
a woman standing or seated upright in a specialized evaluation
chair. During testing, two catheters are used. One is placed into
the bladder and the other into either the vagina or rectum. The
vagina is preferred unless advanced prolapse is evident, as stool
in the rectal vault may obstruct catheter sensors and lead to
inaccurate readings. Additionally, vaginal placement for most
women is more comfortable. From each of these two catheters, distinct pressure readings are obtained or calculated and
include: (1) intraabdominal pressure, (2) vesicular pressure, (3)
calculated detrusor pressure, (4) bladder volume, and (5) saline
infusion flow rate. As shown in Figures 23-15 and 23-16, the
different forms of incontinence can be differentiated.
Uroflowmetry. Initially, women are asked to empty their bladder into a commode connected to a flowmeter (uroflowmetry).
After a maximal flow rate is recorded, the patient is catheterized to
measure a postvoid residual and to ensure an empty bladder prior
to further testing. This test provides information on a woman’s
ability to empty her bladder and can identify women with urinary retention and other types of voiding dysfunction. Presuming
that a patient begins with a comfortably full bladder of 200 mL
or greater, most patients can empty their bladders over 15 to
20 seconds with flow rates of greater than 20 mL/sec. Maximum
flow rates of less than 15 mL/sec, with a voided volume greater
than 200 mL, are generally considered abnormally slow. In this
setting—especially if accompanied by urinary retention—voiding
dysfunction is identified. This may result from obstruction from
a kinked urethra in the setting of anterior vaginal wall prolapse or
postoperatively after creation of antiincontinence support that is
too tight. Voiding dysfunction may also occur in settings of neurologic dysfunction with poor detrusor contractility, as in those
with poorly controlled diabetes.
Cystometrography. Following uroflowmetry, cystometrography is performed to determine whether a woman has urodynamic stress incontinence (USI) or detrusor overactivity
(DO). Additionally, this test provides information on bladder
threshold volumes at which a woman senses bladder capacity.
Delayed sensation or sensation of bladder fullness only with
large capacities may indicate neuropathy. Conversely, extreme
bladder sensitivity may suggest sensory disorders such as interstitial cystitis.
For the cystometrogram, a catheter is inserted transurethrally
into the bladder and a second catheter is inserted into the vagina
or rectum (see Fig. 23-15). While the patient is seated, the bladder is filled with room-temperature sterile normal saline, and
CHAPTER 23
bladder through the same catheter until approximately 300 mL
is used or until a subjective maximum capacity is reached. The
patient is then asked to void spontaneously into a urine collection device. The difference between volume infused and volume
retrieved is recorded as the PVR. A residual of less than 100 mL or
less than one third of the instilled volume—if less than 300 mL is
infused—is consistent with adequate bladder emptying.
621
622
Female Pelvic Medicine and Reconstructive Surgery
Urethra
Bladder catheter
SECTION 3
Pabd
Pves
Pves
Pdet
Pabd
Pves = Pabd + Pdet
Pdet = Pves – Pabd
Vaginal/rectal catheter
Vagina/rectum
a.
b.
Leakage
+
–
Diagnosis
USI
No
USI
Clinical scenario
I
II
a.
b.
Pabd (abdominal pressure)
[vaginal/rectal catheter]
Pves (bladder pressure)
[bladder catheter]
Pdet (true detrusor pressure)
[subtracted/calculated]
+
or
DO
–
+
or
–
DO
FIGURE 23-15 Interpretation of multichannel urodynamic evaluation: cystometrogram. A catheter is placed in the bladder to determine the pressure generated within it (Pves). The pressure in the bladder is produced from a combination of the pressure from the
abdominal cavity and the pressure generated by the detrusor muscle of the bladder. Bladder pressure (Pves) ϭ pressure in abdominal
cavity (Pabd) ϩ detrusor pressure (Pdet). A second catheter is placed in the vagina (or rectum if advanced-stage prolapse is present) to
determine the pressure in the abdominal cavity (Pabd). As room-temperature saline is instilled into the bladder, the patient is asked to
cough every 50 mL and the external urethral meatus is observed for leakage of urine around the catheter. The volume at first desire
to void and the bladder capacity is recorded. Additionally, the detrusor pressure (Pdet) channel is observed for positive deflections to
determine if there is detrusor activity during testing. The detrusor pressure (Pdet) cannot be measured directly by any of the catheters.
However, from the first equation, we can calculate the detrusor pressure (Pdet) by subtracting the abdominal pressure (Pabd) from the
bladder pressure (Pves):
Detrusor pressure (Pdet) ϭ bladder pressure (Pves) Ϫ pressure in abdominal cavity (Pabd)
I. Urodynamic Stress Incontinence (USI)
Urodynamic stress incontinence is diagnosed when urethral leakage is seen with increased abdominal pressure, in the absence of detrusor pressure.
a. ϩUSI (Column 1): Abdominal pressure is generated with Valsalva maneuver or cough. This pressure is transmitted to the bladder, and
a bladder pressure (Pves) is noted. The calculated detrusor pressure is zero. Leakage is observed, and diagnosis of USI is assigned.
b. No USI (Column 2): Abdominal pressure is generated with Valsalva maneuver or cough. This pressure is transmitted to the bladder,
and a bladder pressure (Pves) is noted. The calculated detrusor pressure is zero. Leakage is not observed. The patient is not diagnosed as
having USI.
II. Detrusor Overactivity (DO)
Detrusor overactivity is diagnosed when the patient has involuntary detrusor contractions during testing with or without leakage.
a. ϩDO (Column 3): Although no abdominal pressure is observed, a vesicular pressure is noted. A calculated detrusor pressure is
recorded and noted to be present. A diagnosis of DO is made regardless of whether leakage is seen.
b. ϩDO (Column 4): In this example, an abdominal pressure is observed as well as a vesicular pressure. Using only the Pabd and the Pves
channels, it is difficult to tell whether or not the detrusor muscle contributed to the pressure generated in the bladder. On subtraction, a
calculated detrusor pressure is recorded. Thus, a diagnosis of DO is made, again regardless of whether leakage is seen.
In addition to these channels, occasionally a channel to detect electromyographic activity is used.
Pabd ϭ pressure in abdominal cavity; Pdet ϭ detrusor pressure (calculated); Pves ϭ bladder pressure.
the patient is asked to cough at regular intervals. Additionally,
during filling, the volumes at which a first desire to void and
maximal bladder capacity is reached are noted. From pressure
readings, DO and/or USI may be identified.
After cystometrography, once approximately 200 mL of
saline has been instilled, an abdominal leak point pressure is
measured. The patient is asked to perform a Valsalva maneuver,
and the pressure generated by the effort is measured and evidence
of urine leakage is sought. If leakage is seen when a pressure of
Ͻ60 cm H2O is generated, then criteria have been met for a
diagnosis of intrinsic sphincteric deficiency. At our institution,
abdominal leak point pressures are measured at a bladder volume
Urinary Incontinence
A. Normal bladder
response
80
Cough
Valsalva
C. Urodynamic stress
incontinence
D. Normal
voiding
Cough
0
80
Bladder catheter 60
(bladder
40
pressure)
cm H2O
20
0
80
Subtracted
60
pressure
(true detrusor 40
pressure)
20
cm H2O
0
Detrusor
overactivity
40
30
Flow rate
20
(mL/sec)
10
0
↑ Leak visualized
↑ Leak visualized
TIME
FIGURE 23-16 Urodynamic testing. Cystometrography is reflected by parts A, B, and C. A. In a patient with normal function, note that
provocation by coughing or Valsalva maneuver does not provoke an abnormal rise in detrusor pressure. B & C. In a patient with combined
detrusor overactivity and urodynamic stress incontinence. First, spontaneous detrusor activity leads to increased bladder pressure reading
in the absence of cough or Valsalva maneuver. Second, a cough alone leads to urine leakage, independent of detrusor muscle activity.
D. Pressure flowmetry. At maximum capacity and on command, a detrusor contraction is generated, and voiding is initiated.
of 200 mL, using the true zero of intravesical pressure as the baseline. However, the volume at which this test is performed varies
among institutions, with some choosing to use bladder capacity
and others choosing to use 150 mL as the testing volume.
Pressure Flowmetry. This evaluation usually follows cystometrography and is similar to the uroflowmetry conducted
at the beginning of urodynamic testing. A woman is asked to
void into a large beaker that rests on a calibrated weighted sensor. Maximum flow rate and postvoid residual are once again
recorded. Similar to uroflowmetry, the output from the urodynamics instrumentation provides a graphical representation of
the void. However, during voiding, a woman now has a microtip transducer catheter in her bladder, which provides an additional display of detrusor pressure during the void, including
at the point of maximum flow rate. This is particularly useful
in women who may have incomplete bladder emptying, as the
pressure flowmetry may suggest either an obstructive scenario
(elevated maximal detrusor pressure with slow flow rate) or poor
detrusor contractility (low detrusor pressure and slow flow rate).
Urethral Pressure Profile. The final part of cystometric testing is the urethral pressure profile. At our institution, we usually perform this test in the seated patient with a volume of
200 mL instilled in the bladder. However, again, this volume
is often institution dependent. A catheter transducer is positioned within the bladder, and the microtip dual-sensor catheter is pulled through the urethra with the aid of an automated
puller arm at a speed of 1 mm/sec. Maximum urethral closure
pressure (MUCP) is determined by averaging three pressure
profiles. The functional urethral length and the area of continence zone are also obtained. These values provide important
information on the intrinsic properties of the urethra and aid in
the diagnosis of ISD. A diagnosis of ISD is made if the MUCP
is Յ20 cm H2O or as described in the last section, if the leak
point pressure is Ͻ60 cm H2O (McGuire, 1981). These terms
and concepts provide the rationale for procedures aimed at correcting stress incontinence. Importantly, however, the values
used to define ISD are not well standardized and have not been
consistently found to influence surgical outcomes (Monga,
1997; Weber, 2001).
CHAPTER 23
Vaginal catheter 60
(abdominal
40
pressure)
cm H2O
20
B. Detrusor
overactivity
623
624
Female Pelvic Medicine and Reconstructive Surgery
TREATMENT
■ Conservative/Nonsurgical
SECTION 3
Pelvic Floor Strengthening Exercises
Conservative management is a reasonable initial approach to
most patients with urinary incontinence. The rationale behind
conservative management is to strengthen the pelvic floor and
provide a supportive “backboard” against which the urethra
may close. Options include active pelvic floor exercises and passive electrical pelvic floor muscle stimulation. For both SUI and
urge urinary incontinence, these fundamentals prove valuable.
With SUI, pelvic floor strengthening attempts to compensate
for anatomic defects. For urge urinary incontinence, it improves
pelvic floor muscle contraction strength to provide temporary
continence during waves of bladder detrusor contraction.
Pelvic Floor Muscle Training. In women who have mild to
moderate symptoms, pelvic floor muscle training (PFMT) may
improve if not cure urinary incontinence. Also known as Kegel
exercises, PFMT entails voluntary contraction of the levator ani
muscles. As with any muscle building, isometric or isotonic
forms of exercise may be selected. Exercise sets should be performed numerous times during the day, with some reporting up
to 50 or 60 times each day. However, specific details in performance of these exercises are subject to provider preference and
clinical setting.
If isotonic contractions are used for PFMT, a woman is
asked to squeeze and hold contracted levator ani muscles.
Women, however, often have difficulty isolating these muscles.
Frequently, patients will erroneously contract their abdominal
wall muscles rather than the levators. To help localize the correct
group, an individual may be instructed to identify the muscles
that are tightened when snug pants are pulled up and over her
hips. Moreover, in an office setting, a provider can determine if
the levator ani group is contracted by placing two fingers in the
vagina while Kegel exercises are performed.
At our institution, we aim to help patients achieve a sustained
pelvic floor contraction of 10 seconds. We begin with the duration of contraction a patient can sustain (e.g., 3 seconds), and
ask them to hold for this long and then relax for one to two
times this duration (e.g., 6 seconds). This squeeze and release
is repeated 10 to 15 times. Three sets are performed throughout the day for a total of approximately 45 contractions. Over
a series of weeks with frequent follow-up visits, the duration of
contraction is steadily increased. Patients, thus, improve the tone
of their pelvic floor muscles and are usually able to more forcefully squeeze their muscles in anticipation of sudden increases of
intraadominal pressure for SUI.
Alternatively, if isometric contractions are used for PFMT, a
woman is asked to rapidly contract and relax the levators. These
“quick flicks” of the pelvic floor muscles may prove advantageous if waves of urinary urgency strike. Of note, there is a misconception about the value of stopping urination midstream.
Women should be counseled that this practice often worsens
voiding dysfunction.
To augment exercise efficacy, weighted vaginal cones or
obturators may be placed into the vaginal during Kegel exercises.
These provide resistance against which pelvic floor muscles can
work.
Reviewers of the Cochrane database have assessed the effects
of PFMT for women with urinary incontinence compared with
no treatment, placebo or sham treatments, or other inactive
control treatments. Although interventions varied considerably,
women who performed PFMT were more likely to report cure
or improved incontinence and improved continence-specific
quality of life than women who did not use PFMT. The exercising women also objectively demonstrated less leakage during
office-based pad testing (Dumoulin, 2010). Prognostic indicators that may predict a poor response to PFMT for the treatment
of SUI include severe baseline incontinence, prolapse beyond the
hymenal ring, prior failed physiotherapy, a history of prolonged
second stage of labor, BMI Ͼ30 kg/m2, high psychological distress, and poor overall physical health (Hendriks, 2010).
Electrical Stimulation. As an alternative to active pelvic
floor contraction, a vaginal probe may be used to deliver lowfrequency electrical stimulation to the levator ani muscles.
Although the mechanism is unclear, electrical stimulation may
be used to improve either SUI or urge urinary incontinence
(Indrekvam, 2001; Wang, 2004). With urge urinary incontinence, traditionally a low frequency is applied, whereas for
SUI, higher frequencies are used. Electrical stimulation may
be used alone or more commonly in combination with PFMT.
Biofeedback Therapy. Many behavioral techniques, often
considered together as biofeedback therapy, measure physiologic
signals such as muscle tension and then display them to a patient
in real time. In general, visual, auditory, and/or verbal feedback
cues are directed to the patient during these therapy sessions.
Specifically, during biofeedback for PFMT, a sterile vaginal
probe that measures pressure changes within the vagina during
levator ani muscle contraction is typically used. Visual readings
reflect an estimate of muscle contraction strength. Treatment
sessions are individualized, dictated by the underlying dysfunction, and modified based on response to therapy. In many cases,
reinforcing sessions at various subsequent intervals may also
prove advantageous.
Dietary
Different food groups that may have high acidity or caffeine
content may lead to greater urinary frequency and urgency.
Dallosso and colleagues (2003) found consumption of carbonated drinks to be associated with development of urge
urinary incontinence symptoms. Accordingly, elimination of
these dietary irritants may prove beneficial for these women.
In addition, certain dietary supplements such as calcium glycerophosphate (Prelief) have been shown to decrease urgency
and frequency symptoms (Bologna, 2001). This is a phosphatebased product and is thought to buffer urine acidity.
Scheduled Voiding
Women with urge urinary incontinence may feel voiding urges
as frequently as every 10 to 15 minutes. Initial goals extend voidings to half-hour intervals. Tools used to achieve this include
Kegel exercises during waves of urgency or mental distraction
Urinary Incontinence
Estrogen Replacement
Estrogen has been shown to increase urethral blood flow and
increase ␣-adrenergic receptor sensitivity, thereby increasing urethral coaptation and urethral closure pressure. Hypothetically,
estrogen may also increase collagen deposition and increase vascularity of the periurethral capillary plexus. These are purported
to improve urethral coaptation. Thus, for incontinent women
who are atrophic, administration of exogenous estrogen is reasonable.
Estrogen is commonly administered topically, and many
different regimens are appropriate. At our institution, we use
conjugated equine estrogen cream (Premarin cream) administered daily for 2 weeks, then twice weekly thereafter. Although
no data are available to address the duration of treatment,
women may be treated chronically with topical estrogen cream.
Alternatively, oral estrogen may be prescribed if other menopausal symptoms for which estrogen would be beneficial coexist
(Chap. 22, p. 584).
However, despite these suggested benefits, a consensus
regarding estrogen’s beneficial effects on the lower urinary tract
has not been reached. Specifically, some studies have shown
worsening or development of urinary incontinence with systemic estrogen administration (Grady, 2001; Grodstein, 2004;
Hendrix, 2005; Jackson, 2006).
■ Treatment of Stress Urinary Incontinence
Medications
Pharmaceutical treatment plays a minor role in the treatment
of women with SUI. However, for women with mixed urinary
incontinence, a trial of imipramine is reasonable to aid urethral
contraction and closure. As discussed earlier, this tricyclic antidepressant has ␣-adrenergic effects, and the urethra contains a
high content of these receptors.
Duloxetine (Cymbalta), a selective serotonin- and norepinephrine-reuptake inhibitor (SSRI), has been evaluated for SUI
treatment. In animal studies, serotonergic agonists suppress
parasympathetic activity and enhance sympathetic and somatic
activity. The sum effect promotes urine storage by relaxing the
bladder and increasing outlet resistance. Although considered
investigational, in randomized studies, this SSRI has improved
symptoms in women with SUI (Dmochowski, 2003a; Millard,
2004; Norton, 2002). Moreover, Ghoniem and coworkers
(2005), in a randomized controlled trial, evaluated the benefits of duloxetine, PFMT, and placebo combinations. Pad and
quality-of-life data found the combination of duloxetine and
PFMT to be more effective than either alone.
Previously, phenylpropanolamine (PPA) was used to treat
SUI. However, in 2005, the Food and Drug Administration
(FDA) (2009) reclassified PPA as Category II and considered it
not generally safe or effective. Specifically, the FDA’s decision
was prompted by an increased rate of hemorrhagic strokes suffered by women taking this medication.
Pessary and Urethral Inserts
Certain pessaries have been designed to treat incontinence as
well as pelvic organ prolapse. Incontinence pessaries are designed
to reduce downward excursion or funneling of the urethrovesical junction (Fig. 24-17, p. 648). This provides bladder neck
support and thereby helps to reduce incontinence episodes.
Dependent on the amount of prolapse present, pessary efficacy
for urinary incontinence is variable. Not all women are appropriate candidates for pessaries, nor will all desire long-term
management of incontinence or prolapse with these devices.
A large prospective trial comparing incontinence pessaries
and behavioral therapy for women with SUI demonstrated that
40 and 49 percent of patients were either much or very much
improved at 3 months, respectively. The women randomized
to behavioral therapy reported greater treatment satisfaction,
and a greater percentage reported no bothersome incontinence
symptoms (Richter, 2010b).
As an alternative to pessaries, a urethral insert may also be
used for SUI control. The only currently commercially available
device is the FemSoft Insert. As the device is inserted, its sleeve
slides into and conforms to the urethra and creates a seal at
the bladder neck to prevent accidental urine leakage. During
routine bathroom visits, the insert is removed, discarded, and
replaced with a fresh insert. Data are limited on the effectiveness of this insert. However, in an observational study of 150
women, Sirls and associates (2002) found significantly reduced
rates of incontinence episodes.
Surgical Treatment of Intrinsic
Sphincteric Deficiency
Urethral Bulking Agents. Injection of bulking agents has
been traditionally indicated for women who have stress incontinence associated with intrinsic sphincteric deficiency. However,
the FDA has broadened the criteria for use of bulking agents
to include patients with less severe leak point pressures. As a
result, those with leak point pressures Ͻ100 cm H2O may
also be suitable candidates (McGuire, 2006). Additionally, this
office procedure is a useful alternative for women with SUI
who have multiple medical problems and are thus poor surgical candidates.
Agents are injected into the urethral submucosa to “bulk
up” the mucosa and improve coaptation. Ideally, these injectable bulking agents should be easy to place, effective, durable,
safe, and nonimmunogenic. Since few agents satisfy all of these
characteristics, newer agents are constantly being developed.
The injection location around and along the length of the urethra can vary. Some recommend two locations on either side of
the urethra, whereas others advocate injections in three or four
quadrants. At our institution, we usually inject at the level of
the urethrovesical junction at sites of apparent urethral mucosal defects. However, if a global defect is noted or if a discrete
defect is absent, then a two- to four-quadrant approach is used.
The specific steps of injection and types of products used are
described in Section 43-6 (p. 1198).
CHAPTER 23
techniques during these times. Scheduled voiding, although
used primarily for urge urinary incontinence, may also be helpful for those with SUI. For these patients, regularly scheduled
urination leads to an empty bladder during a greater percentage
of the day. Because some women will leak urine only if bladder volumes surpass specific volumes, frequent emptying can
significantly decrease incontinence episodes.
625
626
Female Pelvic Medicine and Reconstructive Surgery
TABLE 23-5. Summary of Incontinence Procedures
SECTION 3
Procedure
Description
Indication
Comments
Urethral Injection
Bulking agent into urethral
submucosa
ISD
Also for SUI in poor surgical candidates; may
require a number of repeated injections
Needle suspension
Proximal urethra suspended by
anterior abdominal wall
SUI
Low long-term success rates; no longer
recommended for SUI
Paravaginal defect
repair
Lateral vaginal wall attached
to ATFP
Vaginal prolapse
No longer recommended for SUI
Retropubic
urethropexy
Pubocervical fascia attached to:
Cooper ligament (Burch) or
to symphysis pubis (MMK)
SUI
Effective long-term treatment; requires
surgeon experience; less reproducible
benefits than midurethral sling procedure
Pubovaginal slings
Bladder neck supported by
fascial strip attached to
anterior abdominal wall
ISD; failed SUI
procedure
Effective long-term treatment; may be useful
in patients in whom synthetic material is
not desirable; requires isolation of graft
from anterior abdominal wall or from leg
fascia lata
Midurethral slings:
Midurethra supported by
mesh placed :
by retropubic approach or
by transobturator approach
TVT
TOT
SUI; ISD
SUI
Effective short-term treatment, rapid
postoperative recovery; TVT with
long-term efficacy data; further study
required to determine effectiveness of
TOT in patients with ISD
ATFP ϭ arcus tendineus fascia pelvis; ISD ϭ intrinsic sphincteric deficiency; MMK ϭ Marshall-Marchetti-Krantz procedure;
SUI ϭ stress urinary incontinence; TOT ϭ transobturator tape; TVT ϭ tension-free vaginal tape.
Surgical Treatment of Anatomic
Stress Incontinence
For those who are not adequately improved with or do not
desire conservative management, surgery may be an appropriate next step for successful treatment of stress incontinence. As
noted earlier, urethral support is integral to continence. Thus,
surgical procedures that recreate this support often diminish or
cure incontinence. More than 200 procedures have been developed for the surgical correction of SUI, although the complete
physiology underlying their success is not entirely clear. In general, these surgical procedures are believed to prevent bladder
neck and proximal urethra descent during increases in intraabdominal pressure (Table 23-5).
Transvaginal Needle Procedures and Paravaginal Defect
Repair. Surgeries that correct urethral hypermobility are theorized to prevent bladder neck and proximal urethra descent during increases in intraabdominal pressure. In the 1960s through
1980s, needle suspension procedures such as the Raz, Pereyra,
and Stamey techniques were popular surgical treatments for SUI
but have now largely been replaced by other methods. In brief,
these surgeries used specially designed ligature carriers to place
sutures through the anterior vaginal wall and/or periurethral tissues and suspend them to various levels of the anterior abdominal
wall. These relied on the strength and integrity of the periurethral
tissue and abdominal wall strength for successful suspension.
Although initial cure rates were satisfactory, the durability of
these procedures decreased with time. Success rates range from
50 to 60 percent, well below rates found with other current
antiincontinence procedures (Moser, 2006). Failure stemmed
largely from “pull-through” of sutures at the level of the anterior
vaginal wall.
In addition, abdominal paravaginal defect repair (PVDR) is
a surgical procedure that corrects lateral support defects of the
anterior vaginal wall. The technique involves suture attachment
of the lateral vaginal wall to the arcus tendineus fascia pelvis.
Currently, PVDR is primarily a prolapse-correcting operation.
Although previously used to correct SUI, long-term data have
shown this to no longer be a superior method for primary treatment of SUI (Colombo, 1996; Mallipeddi, 2001).
Retropubic Urethropexy. This group of procedures
includes the Burch and Marshall-Marchetti-Krantz (MMK)
colposuspension procedures, which involve suspension and
anchorage of the pubocervical fascia to the musculoskeletal
framework of the pelvis (Section 43-2, p. 1189). Long considered the gold standard for surgical treatment of SUI, the
Burch technique uses the strength of the iliopectineal ligament (Cooper ligament) to lift the anterior vaginal wall and
the periurethral and perivesicular fibromuscular tissue. In
contrast, during MMK surgery, the periosteum of the symphysis pubis is used to suspend these tissues.
The retropubic urethropexy is an effective surgical treatment
of SUI, with 1-year overall continence rates between 85 and
90 percent and with a 5-year continence rate of approximately
70 percent (Lapitan, 2009). Complications commonly associated
with these procedures can include de novo detrusor overactivity,
urinary retention, and in the case of the MMK, osteitis pubis. In
Urinary Incontinence
Pubovaginal Slings. This surgery is a standard procedure
for SUI. It has traditionally been used for SUI stemming from
intrinsic sphincteric deficiency. In addition, this procedure may
also be indicated for patients with prior failed antiincontinence
operations.
With this surgery, a strip of either rectus fascia or fascia lata
is placed under the bladder neck and through the retropubic
space. The ends are secured at the level of the rectus abdominis fascia (Section 43-5, p. 1196). Previously, cadaveric fascia
was used as the suspension material. However, this tissue is
eventually degraded and found not to be durable over time
(FitzGerald, 1999; Howden, 2006). Currently, autologous fascia is preferred and is obtained from the patient’s rectus sheath,
although fascia lata from the thigh is an alternative.
Midurethral Slings. These slings surged onto the market in
the late 1990s, and their therapeutic mechanism is based on the
integral theory hypothesized by Petros and Ulmsten (1993). In
brief, control of urethral closure involves the interplay of three
structures: the pubourethral ligaments, the suburethral vaginal
hammock, and the pubococcygeus muscle. Loss of these support structures is believed to result in urinary incontinence and
pelvic floor dysfunction. These slings are believed to reproduce
the support provided by these ligamentous support structures.
There are many different variations of these procedures,
but all involve midurethral placement of synthetic mesh.
Simplistically, they are classified according to the route of placement and can be subdivided into those using a retropubic or a
transobturator approach. Of these, popular procedures include:
(1) tension-free vaginal tape (TVT), a retropubic method; and
(2) transobturator tape (TOT), a transobturator method.
Midurethral slings provide several advantages. First, these
techniques are effective, and short-term cure rates approximate
90 percent (Lim, 2006). Of the two, retropubic and transobturator approaches appear to offer comparable short-term continence results (de Tayrac, 2004; Morey, 2006). Laurikainen and
coworkers (2007) randomly assigned 267 women to undergo
either type and found equal rates of subjective and objective cure.
Despite favorable comparisons, abundant long-term data
regarding the efficacy of transobturator approaches are lacking.
However, data obtained 17 months postoperatively showed an
incontinence improvement rate of 89 percent for those with
preoperative SUI (Juma, 2007). In contrast, long-term continence rates are known with the retropubic technique, and these
approximate 80 percent (Nilsson, 2004).
In addition to their efficacy, recovery from midurethral
sling placement is rapid, and many gynecologists provide
this surgery on an outpatient basis. However, as with other
antiincontinence surgeries, general risks for midurethral sling
procedures include urinary retention, lower urinary tract and
vascular injuries, and creation of de novo voiding dysfunction
such as urgency and retention.
Retropubic Approach. There are several commercial kits available for this procedure, and one commonly used technique is
the tension-free vaginal tape (TVT). Completed bilaterally, one
trocar is placed through a vaginal suburethral incision lateral
to the urethra and brought out suprapubically through a skin
incision (Section 43-3, p. 1191). Alternatively, needles may be
placed through the retropubic space and into the vagina, in a
“top-down” approach.
A prospective observational study conducted at three centers
in Sweden and Finland confirmed the long-term safety and efficacy of the TVT device, with a 77-percent cure rate at 11.5 years
(Nilsson, 2008). Complications vary depending on institution
and surgeon expertise and include: urgency, mesh erosion, urinary retention, de novo urge urinary incontinence, and vascular,
bowel, and lower urinary tract injury. Of these, bladder perforation is one of the most common, and associated rates range from
3 to 9 percent (Agostini, 2006; Tamussino, 2001; Ward, 2004).
Transobturator Approach. The transobturator (TOT)
approach to midurethral sling placement was introduced with
the intent to reduce the risks of vascular and lower urinary
tract injury that can be associated with traversing the retropubic space. Various kits for this approach are available. Each
contains variations in needle and mesh design, but in general,
a permanent sling material, usually polypropylene, is placed.
Sling material is directed bilaterally through the obturator foramen and underneath the midurethra. The entry point overlies
the proximal tendon of the adductor longus muscle.
The two major types of TOT procedures are defined by
whether needle placement begins inside the vagina and is
directed outward, termed an in-to-out approach, or alternatively starts outside and is directed inward, called an out-toin approach (Section 43-4, p. 1194). Initially, this procedure
was developed with an out-to-in approach. However, with this
direction, bladder and urethral injury were potential complications. In a retrospective study, Abdel-Fattah and colleagues
(2006) compared these two approaches. Injury to the bladder
or ureter complicated 1 percent of nearly 400 procedures, and
all followed the out-to-in technique.
As a result, the in-to-out approach was created and marketed
with the assertion of decreased lower urinary tract injury rates.
However, with the in-to-out technique, the trocar tip travels
closer to the obturator neurovascular bundle (Achtari, 2006;
Zahn, 2007). Thus, although each method has its theoretical
advantages, the possibility of injury is not entirely eliminated.
The transobturator approach provides an effective daysurgery technique with potentially lower rates of bladder injury.
However, some retrospective studies have suggested that it may
have limited effectiveness for patients who demonstrate urodynamic criteria for intrinsic sphincteric deficiency (Miller, 2006;
O’Connor, 2006). Prospective randomized comparative studies
are needed to clarify the efficacy of each transobturator midurethral sling and to confirm the relative safety of each technique.
A multicenter randomized study of 597 women compared the
retropubic and transobturator techniques for treatment of SUI.
No significant differences in objective and subjective success
rates at 12 months were found between the retropubic (80.8
and 62.2 percent) and the transobturator (77.7 and 55.8 percent) routes of surgery. The retropubic route had a significantly
higher rate of postoperative voiding dysfunction requiring
reoperation, whereas the transobturator route resulted in more
CHAPTER 23
addition, data suggest that performing a Burch retropubic urethropexy concurrently with abdominal sacrocolpopexy for vaginal vault prolapse may significantly reduce rates of symptomatic
postoperative SUI (Chap. 24, p. 655) (Brubaker, 2008a).
627
628
Female Pelvic Medicine and Reconstructive Surgery
neurologic symptoms. Overall quality of life and satisfaction
with the two procedures were similar (Richter, 2010a).
SECTION 3
Minimally Invasive Slings. Modification of the TVT and
TOT procedure is seen with the minimally invasive slings, sometimes called “microslings” or “minislings.” With this technique,
an 8-cm-long strip of polypropylene synthetic mesh is placed
across and beneath the midurethra through a small vaginal incision. Mesh is not threaded through the retropubic space and
avoids the potential for vascular injury. Currently, the only minimally invasive sling with published data is the TVT-Secur. Initial
results have suggested high objective and subjective cure rates
(Neuman, 2008). Unfortunately, most of these studies have been
case series without comparison or control groups. Additionally,
some studies have reported complications such as recurrent UTI
(10 percent), de novo urge urinary incontinence (10 percent),
and voiding difficulty (8 percent) (Meschia, 2009). Moreover,
lower urinary tract injury is not completely averted with this
method. As with most technology, data from well-conducted,
long-term comparative studies on efficacy and safety should be
obtained before complete adoption of any new technique.
Other techniques that have been introduced include microwave ablation of the periurethral tissues. However, current data
do not support the efficacy or safety of this method.
■ Treatment of Urge Urinary Incontinence
Anticholinergic Medications
These medications appear to work at the level of the detrusor
muscle by competitively inhibiting acetylcholine at muscarinic
receptors (M2 and M3) (Miller, 2005). These agents thereby
blunt detrusor contractions to reduce the number of incontinence episodes and volume lost with each. These medications
are significantly better than placebo at improving symptoms of
urge urinary incontinence and overactive bladder. However, in a
Cochrane database review, Nabi and colleagues (2006) reported
that the reduction in baseline urgency incontinence episodes per
day reflects only a modest margin of benefit.
Oxybutynin, Tolterodine, and Fesoterodine. These commonly used drugs competitively bind to cholinergic receptors
(Table 23-6). As discussed earlier, muscarinic receptors are
TABLE 23-6. Pharmacologic Treatment of Overactive Bladder
Drug Name
Brand Name
Drug Type
Dosage
Available Doses
Oxybutynin (short-acting)
Ditropan
Antimuscarinic
2.5–5 mg PO tid
5-mg tablet,
5 mg/mL syrup
Oxybutynin (long-acting)
Ditropan XL
See above
5–30 mg PO daily
5-, 10-, 15-mg tablet
Oxybutynin (transdermal)
Oxytrol
See above
3.9 mg/d; patch changed
twice weekly
36-mg patch,
8 per carton
Oxybutynin (transdermal)
10% gel
Gelnique
See above
Gel applied 1 g daily
1-g packet,
30 per carton
1-g pump dose,
30 doses per bottle
Tolterodine (short-acting)
Detrol
See above
1–2 mg PO bid
1-, 2-mg tablet
Tolterodine (long-acting)
Detrol LA
See above
2–4 mg PO daily
2-, 4-mg capsule
Fesoterodine fumarate
Toviaz
See above
4–8 mg PO daily
4-, 8-mg tablets
Trospium chloride
Sanctura
Antimuscarinic
quaternary amine
20 mg PO bid
20-mg tablet
Trospium chloride
Sanctura XR
See above
60 mg PO daily
60-mg tablet
Darifenacin
Enablex
M3-selective
antimuscarinic
7.5–15 mg PO daily
7.5-, 15-mg tablet
Solifenacin
Vesicare
M3-selective
antimuscarinic
5–10 mg PO daily
5-, 10-mg tablets
Imipramine hydrochloride
Tofranil
Tricyclic antidepressant,
anticholinergic,
␣-adrenergic,
antihistamine
10–25 mg PO qd-qid
10-, 25-, 50-mg
tablets
bid ϭ twice daily; PO ϭ orally; qd ϭ daily; qid ϭ four times daily; tid ϭ three times daily.
Urinary Incontinence
TABLE 23-7. Potential Anticholinergic Side Effects
Potential Clinical Consequence
Increased pupil size
Photophobia
Decreased visual
accommodation
Blurred vision
Decreased salivation
Gingival and buccal ulceration
Decreased bronchial
secretions
Small-airway mucus plugging
Decreased sweating
Hyperthermia
Increased heart rate
Angina, myocardial infarction
Decreased detrusor
function
Bladder distension and urinary
retention
Decreased
gastrointestinal
mobility
Constipation
not limited to the bladder. Thus, side effects with these drugs
may be significant. Of these, dry mouth, constipation, and
blurry vision are the most common (Table 23-7). Patients
frequently report that dry mouth is a primary reason for
drug discontinuation. Importantly, anticholinergics are contraindicated in those with narrow-angle glaucoma. Because
of these effects, the therapeutic goal of bladder M3 blockade
with these antimuscarinic agents is often limited by their anticholinergic side effects. Accordingly, drug selection should
be tailored, and efficacy is balanced against tolerability. For
example, Diokno and associates (2003) found oxybutynin to
be more effective than tolterodine. However, tolterodine was
associated with lower side effect rates. Tolterodine and fesoterodine have also been compared in a randomized study of
1135 patients. Fesoterodine was found to perform above tolterodine, although once again, side effects were lowest in the
tolterodine group (Chapple, 2008). A population-based study
reported that only 56 percent of women felt their overactive
bladder medication was effective, and half stopped taking the
medication (Diokno, 2006).
Most side effects attributed to oxybutynin stem from its secondary metabolite that follows liver metabolism. Therefore, to
minimize oral oxybutynin side effects, a transdermal patch was
designed to decrease the “first-pass” effect of this drug. This
leads to decreased liver metabolism and fewer systemic cholinergic side effects. Dmochowski and coworkers (2003b) found
fewer anticholinergic side effects with transdermal oxybutynin
compared with long-acting oral tolterodine.
Transdermal oxybutynin (Oxytrol) is supplied as a 7.6 ϫ
5.7 cm patch that is applied twice weekly to the abdomen,
hip, or buttock. Each patch contains 36 mg of oxybutynin and
delivers approximately 3.9 mg each day. Application-site pruritus is the most common side effect, and varying the application
site may minimize skin reactions (Sand, 2007). A newer trans-
Imipramine. This agent is less effective than tolterodine
and oxybutynin but displays ␣-adrenergic and anticholinergic characteristics. Therefore, it is occasionally prescribe for
those with mixed urinary incontinence. Importantly, doses of
imipramine used to treat incontinence are significantly lower
than those used to treat depression or chronic pain. In our
experience, this minimizes the theoretical risk of drug-related
side effects.
Selective Muscarinic-Receptor Antagonists. Newer anticholinergic medications have been introduced that aim to reduce
side effects. The agents are all M3-receptor selective antagonists and include solifenacin (VESIcare), trospium chloride
(Santura), and darifenacin (Enablex). Advantages of increased
urgency warning time and decreased muscarinic side effects have
been shown in randomized controlled studies (Cardozo, 2004;
Chapple, 2005; Haab, 2006; Zinner, 2004). However, although
the side-effect profiles of these drugs are attractive, they have not
been proved superior to nonselective muscarinic-receptor drugs
in randomized controlled trials (Nabi, 2006).
Sacral Neuromodulation
Urine storage and bladder emptying requires a complex coordinated interaction of spinal cord and higher brain centers,
peripheral nerves, urethral and pelvic floor muscles, and the
detrusor muscle. If any of these levels are altered, normal micturition is lost. To overcome these problems, electrical nerve
stimulation, also called neuromodulation, has been used.
InterStim is the only implantable neuromodulation system
approved by the FDA for treatment of refractory urge urinary
incontinence. It is also approved for treatment of anal incontinence. It may be also considered for those with pelvic pain,
interstitial cystitis, and defecatory dysfunction, although it is
not FDA-approved for these indications. Sacral neuromodulation is not considered primary therapy and is generally offered
to women who have typically exhausted pharmacologic and
conservative options.
This outpatient surgically implanted device contains a pulse
generator and electrical leads that are placed into the sacral
foramina to modulate bladder and pelvic floor innervation. Its
mode of action is incompletely understood, but may be related
to an inhibition of somatic afferents that interrupts abnormal
reflex arcs in the sacral spinal cord involved in the filling and
evacuation phases of micturition (Leng, 2005).
Implantation is typically a two-stage process. Initially,
leads are placed and attached to an externally worn generator (Section 43-12, p. 1212). After placement, frequency and
amplitude of electrical impulses can be adjusted and tailored to
maximize effectiveness. If a 50-percent or greater improvement
in symptoms is noted, then internal implantation of a permanent pulse generator is planned. This procedure is minimally
invasive and is typically completed in a day-surgery setting.
CHAPTER 23
Side Effect
dermal 10-percent oxybutynin gel (Gelnique) is applied daily
to skin of the abdomen, upper arms/shoulders, or thigh, and
application sites should be rotated. Each sachet contains a 1-g
dose of oxybutynin chloride gel, which delivers approximately
4 mg of oxybutynin daily (Staskin, 2009).
629