Food safety behavior in primary cook and health outcomes of household in ho chi minh city
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (1.36 MB, 81 trang )
MINISTRY OF EDUCATION AND TRAINING
UNIVERSITY OF ECONOMICS HO CHI MINH CITY
NGO HOANG TUAN HAI
FOOD SAFETY BEHAVIOR IN PRIMARY COOK AND HEALTH
OUTCOMES OF HOUSEHOLD IN HO CHI MINH CITY
MASTER OF ECONOMICS THESIS
Ho Chi Minh City - Year 2016
MINISTRY OF EDUCATION AND TRAINING
UNIVERSITY OF ECONOMICS HO CHI MINH CITY
NGO HOANG TUAN HAI
FOOD SAFETY BEHAVIOR IN PRIMARY COOK AND HEALTH
OUTCOMES OF HOUSEHOLD IN HO CHI MINH CITY
Major: Development Economics
ID: 60310105
MASTER OF ECONOMICS THESIS
SUPERVISOR: DR. PHAM KHANH NAM
Ho Chi Minh City - Year 2016
COMMITMENT
I commit the thesis “Food safety behavior of primary cook and health outcomes
of household in Ho Chi Minh city” is my own research.
Except the references which are extracted in this thesis, there is no any others
research or documents which is used in the thesis against regulatory.
I would bear the full responsibility of my research. The data, conclusion in this
thesis is fidelity and not published in any research yet.
Ho Chi Minh City, October 31st, 2016.
Ngo Hoang Tuan Hai
TABLE OF CONTENT
COMMITMENT
TABLE OF CONTENT
ACKNOWLEDGEMENT
LIST OF ABBREVIATIONS
LIST OF FIGURES
LIST OF TABLES
CHAPTER 1 : INTRODUCTION........................................................................................... 1
1.1 PROBLEM STATEMENTS................................................................................................. 1
1.2 RESEARCH OBJECTIVES AND RESEARCH QUESTIONS .......................................... 6
1.3 SCOPE OF RESEARCH ...................................................................................................... 8
1.4 THESIS STRUCTURE......................................................................................................... 9
CHAPTER 2 : LITERATURE REVIEW .............................................................................10
2.1 FOOD SAFETY AND FOOD-BORNE DISEASES ......................................................... 10
2.2 THE HEALTH BELIEF MODEL: ..................................................................................... 11
2.3 EMPIRICAL REVIEWS ON DRIVERS OF FOOD SAFETY PRACTICES: ................. 13
CHAPTER 3 : RESEARCH METHODOLOGY .................................................................18
3.1 ANALYTIC FRAMEWORK ............................................................................................. 18
3.2 ECONOMETRIC MODELS .............................................................................................. 19
3.3 DATA ................................................................................................................................. 25
CHAPTER 4 : RESEARCH RESULTS ................................................................................28
4.1 FOOD SAFETY PROBLEMS IN VIETNAM ................................................................... 28
4.2 DESCRIPTIVE STATISTICS ............................................................................................ 31
4.3 RESULTS FROM MULTIVARIATE PROBIT MODELS ............................................... 39
4.4 RESULTS FROM PROPENSITY SCORE MATCHING MODEL .................................. 45
CHAPTER 5 : DISCUSSION AND IMPLIED POLICY ....................................................49
5.1 DISCUSSIONS AND CONCLUSIONS ............................................................................ 49
5.2 POLICY IMPLICATION ................................................................................................... 50
5.3 LIMITATION AND IMPLICATIONS FOR FURTHER RESEARCH ............................ 51
Appendix 1: The correlation matrix of perception’s factors ...............................................53
Appendix 2: PCA result ..........................................................................................................54
Appendix 3: MVP regression (reduced form) .......................................................................55
Appendix 4: MVP regression (original form) .......................................................................56
Appendix 5: Poisson regression ..............................................................................................57
Appendix 6: Questionaire form ..............................................................................................58
References .................................................................................................................................67
ACKNOWLEDGEMENT
Firstly, I would like to express my gratitude to Dr Pham Khanh Nam, my
supervisor, for all the suggestions, recommendations, knowledge and guidance that he
did to support me to finish the thesis.
Secondly, I am very grateful to doctor, MPH Nguyen Thi Huynh Mai, vice
director of Safety Hygiene Food Branch of Ho Chi Minh city, for the permission as
well as the advice to use the food safety data.
Thirdly, I would like to thankful to my colleagues, my friend for all the
encouragement and support they gave to me during the thesis processing.
Lastly, my sincere thanks are all to the member of School of Economics –
University of Economic Ho Chi Minh city for their effort to create the best
environment for studying and researching for me as well as other students during the
course.
Ho Chi Minh city, October 31st, 2016.
Ngo Hoang Tuan Hai
LIST OF ABBREVIATIONS
FBD: Food-borne disease
WHO: World Health Organization
FAO: Food and Agriculture Organization
HBM: Heal Belief Model
MVP: Multivariate Probit
KAP: Knowledge, Attitude and Practice
PSM: Propensity Score Matching
CDC: Center for Disease Control and Prevention
LIST OF FIGURES
Figure 1.1: The number of food-borne cases annually (WHO, 2015) ............................. 2
Figure 1.2: The number of death caused by FBD annually (WHO, 2015) ...................... 3
Figure 1.3: The burden of FBD (WHO, 2015) ................................................................ 4
Figure 2.1: Health belief Model Components and Linkages (Glanz et al, 2008) .......... 13
Figure 3.1: The Health Belief Model application in food safety ................................... 19
Figure 4.1: The number of food poisoning cases in Vietnam (MOH, 2016) ................. 28
Figure 4.2: The number of food poisoning outbreaks and death in Vietnam (MOH,
2015)............................................................................................................................... 29
Figure 4.3: The number of food poisoning cases in HCM city (FSBDH, 2016) ........... 30
Figure 4.4: The nonparametric relationship between food safety practice and
knowledge, perception ................................................................................................... 38
LIST OF TABLES
Table 2.1: The concepts of Health Belief Model ........................................................... 11
Table 3.1: Variables’ description ................................................................................... 23
Table 4.1: Demographic characteristics of participants (category variables) ................ 31
Table 4.2: Demographic characteristics of participants (continuous variables) ............ 32
Table 4.3: Factor analysis result..................................................................................... 35
Table 4.4: Food safety practices..................................................................................... 37
Table 4.5: MVP regression reduced form ...................................................................... 39
Table 4.6: MVP regression original form ...................................................................... 41
Table 4.7: Marginal effect after MVP regression .......................................................... 42
Table 4.8: Poisson regression ......................................................................................... 44
Table 4.9: Probit regression result ................................................................................. 46
Table 4.10: Differences of continuous variables ........................................................... 47
Table 4.11: Correlations between binary variables and FBD ........................................ 48
ABSTRACT
Nowadays food safety issue appeals a lot of attention from the global
organization to local authorities. Each year, the food-borne diseases cause an enormous
burden on people heath as well as national’s economy. As climate change suffered
country with the developing economy, Vietnam has to face to many food safety
challenges. In recent years, the Vietnam government has invested much effort in order
to maintain the rate of economic growth while trying to improve the people’s health by
a lot of new law and institutions. However, the food safety policy does not focus on
adjusting the consumer’s behavior. As a result, the impact of individual’s practice on
their health was not determined clearly in Vietnamese community.
This research’s objective is to find out the factors that modify the food safety
practice of household primary food preparer and the effect of these behaviors on food
poisoning risk. The results show that the food safety knowledge and perception have
significant effect on household cook’s practices while their behaviors do not have the
explicit impact on the food poisoning’s risk.
Keywords: food safety, food knowledge, perception and behavior, food poisoning
1
CHAPTER 1 : INTRODUCTION
1.1 PROBLEM STATEMENTS
The agricultural revolution has brought a large amount of food, rations for human
and improved laborer’s health, a fundamental factor of human capital. Therefore, food
safety1 problem would give negative impact to the sustainable development of
developing countries as well as the national’s security. The fact that many diseases
related to food demonstrated recently has driven many countries’ attention from food
quantity to food safety.
The usage of pesticides, chemical fertilizer and feedstuff improve agriculture’s
capacity. However, the overuse and misuse of them affect the quality of food. In
addition, the preservation and processing method as well as food additive exploitation
both make food become less safety. According to WHO (2015), the main factors cause
food-borne disease are bacteria, virus, parasites, chemicals and toxins. The most
dedicated people of food-borne illness are children, pregnant women and the elder.
Due to the development of transportation and international trade, food safety
issue is not only the problem of any countries but also a global problem. For examples:
Chinese milk scandal, New Zealand material milk crisis caused an enormous loss for
the manufacturer and impinge on other countries as well as consumer’s health.
1
World Health Organization (WHO) and Food and Agriculture Organization (FAO) defined:
“Food safety is the assurance that food will not cause harm to the consumer when it is prepared and
eaten according to its intended use” (WHO and FAO, 2009, p. 6).
2
700,000,000
600,000,000
500,000,000
400,000,000
300,000,000
200,000,000
100,000,000
0
Global total
Eastern
Mediterranea
Europe
Western
Pacific
America
South East
Asia
Africa
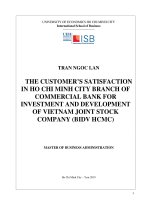
Figure 1.1: The number of food-borne cases annually (WHO, 2015)
FBD occur in all countries in the world. However, the developing regions, such as
South East Asia and Africa, distributed the majority of food-borne cases while the
developed areas, such as Europe and America, had the least number of food-borne
cases. An unexpected result is that although African countries are lack of food source
and food safety control, this region had less amount of food-borne illness cases than the
South East Asian region. The reasons of this phenomenon may be due to the diversity
of high nutrition food and the tropical weather in the Asian area. These two factors are
the ideal condition for bacteria and other food risky factors to affect the human health.
WHO (2015) estimated that every year food-borne disease cause almost 10%
global populations to fall ill and responsible for 420,000 deaths (one third are children).
Among all FBD, diarrheal diseases are the most common illnesses resulting from
3
unsafe food, accounted for half of global burden of FBD and made 550 million people
falling ill (including 220 million children), cause 230,000 deaths (96,000 children’s)
450,000
400,000
350,000
300,000
250,000
200,000
150,000
100,000
50,000
0
Global total
Eastern
Mediterranea
Europe
Western
Pacific
America
South East
Asia
Africa
Figure 1.2: The number of death caused by FBD annually (WHO, 2015)
Similar with the number of food-borne cases, the number of death caused by FBD
showed the same trend. South East Asian and African regions continued to distribute
the largest number of death cases while the European and American had the least
amount of death by FBD. The African region also had less number of death case than
the South East Asian. This consequence may be the effect of many international
medical supports to the Africa than the Asian. In addition, the distinction of physical
strength of local population between these two regions is another fundamental reason.
The FBD caused the burden about 33 million DALYs2. Diarrheal diseases agents
were the largest contributors, accounted for 18 million DALYs, 54% of total. All three
2
DALYs: Disability-adjusted life year, a health gap measure that combines the years of life lost due to
premature death (YLL) and the years lived with disability (YLD) from a disease or condition, for
4
figures 1.1, 1.2, 1.3 both indicated that South East Asian and African region’s food
safety issue is severe and these areas suffered an enormous burden from FBD.
However, despite of the number of death cases in Africa was less than Asia, the
burden of FBD in this area was almost twice than the South East Asian and much more
than other areas. The European, Western Pacific and American total burden was almost
equal to the South East Asia’s and half than the Africa’s burden. These figures exposed
the distance of the health care facilities as well as the food safety controlled policy
between each areas and their impact of population’s health outcomes.
3000
2500
2000
1500
DALYs per 100,000
population
1000
500
0
Figure 1.3: The burden of FBD (WHO, 2015)
varying degrees of severity, making time itself the common metric for death and disability. One DALY
equates to one year of healthy life lost (WHO, 2015).
5
According to the region category of WHO, Vietnam is categorized in the Western
Pacific areas. In the general view of this organization, food-borne illness figure’s of
this area is at the middle level of the world. The similarity result repeated in Vietnam
case. However, this region includes various kinds of countries, from developed
countries such as Australia, Japan, Republic of Korea to the developing ones such as
Cambodia, Philippines, Vietnam. Thus, the contribution of each country has a huge
distinction. The specific information of Vietnam case showed in Chapter 4.
Although the developing countries suffer the most from FBD, the developed
countries also have difficulty with food-borne illness. According to Center for Disease
Control and Prevention (CDC), The USA had 864 food-borne disease outbreaks,
resulting in 13,246 illnesses, 712 hospitalizations, caused 21 deaths, and 21 food
recalls in 2014. In detail, the majority of the food poisoning cases occurred in
restaurant (485 cases, accounted for 65%), followed by private home (86 cases,
accounted for 12%). The most popular causes of food-borne illness in 2014 was
bacteria (149 cases, confirmed and suspected) distributed 22% of total cases. Those
figures proved that even the country with well-organized healthcare system and policy
has to struggle with food poisoning.
CDC also predicted that food safety issue would continue emerge in the future
due to:
-
Changes in our food production and supply, including more imported foods.
-
Changes in the environment leading to food contamination.
-
Better detection of multistate outbreaks.
-
New and emerging bacteria, toxins, and antibiotic resistance.
-
Changes in consumer preferences and habits.
-
Changes in the tests that diagnose foodborne illness.
6
Despite of the wave of immigrants, the increase of trade exchange, the
globalization problem, the food-borne disease is not the attention of any single country
but it is the issue of the modern world.
1.2 RESEARCH OBJECTIVES AND RESEARCH QUESTIONS
1.2.1 Benefits of the research
The diversity of food and food market in Vietnam create the convenience for
household lady to purchase food. Therefore, most of the Vietnamese’s households
often cook and eating at home at least one meal per day. For that reason, as well as the
outside factor’s effects, the people’s behaviors also play an important role in their food
poison possibility. Those behaviors established from their socio-economic statement,
individual characteristics and living condition. In addition, the habit of cooking in
Vietnam community transmitted from generations, thus the Asian tradition and
agricultural culture caused a deep impact on the household cooking behaviors. The role
of tradition and culture expose through the knowledge of food processing, preserving
as well as their practice in the kitchen.
Some research about the Knowledge, Attitude and Practice (KAP) of the people
in Thua Thien Hue province (Duong, 2013), Ho Chi Minh city (Nguyen, 2010) both
indicate the correlation between knowledge, attitude toward food safety and the food
safety practice of individual at food factory, restaurant as well as household. According
to the “10 golden principles in food processing” (MOH, 2005), the food safety
behaviors include:
-
Clean, tidy kitchen and the cooker surface
-
Using waste basket with cover
-
Toilet outside the kitchen
-
Use clean water to handle food
-
Separate well-done food and raw food in processing and preserving
7
-
Use clean tool to prepare and divide food
-
Clean vegetable precisely
-
Not use forbidden food additives or out of date food
-
Washing hand before cooking and after toileting
-
Not smoke, spit out or nail polished while cooking
These golden principles were used frequently in many researches in Vietnam and
were the outcome behavior in this thesis. However, most of these researches were
medical perspective so the socio-economic statement and individual characteristics are
not well considered. As a result, the effect of these factors on food safety behaviors has
not assessed explicitly.
On the other hand, the finding of those research merely indicated the current
statement of food safety issue in the community without the relative analyzing of multi
factors to confirm their impact. Moreover, the participants of the above research did
not participate in the annual survey. In consequence, the effect of government policy
and activities did not mention in the research.
In order to review and confirm the factors which have impact on food safety
behavior, this thesis’s objective is determining these factors as well as estimating their
effect on individual behavior and predict their food-borne disease possibility. These
potential factors include the socio-economic status, the knowledge about food safety,
the perception and the information source of each individual. Whether the personal
causes are determined, the government could develop the compatible strategy to adjust
the people’s behavior, prevent those risky ones, minimized the individual food-borne
diseases possibility in the public and its burden.
1.2.2 General objectives
To analyze food safety behavior and health outcomes of household primary cook
8
1.2.3 Specific objectives
-
To determine the relationship between knowledge, perception of consumer and
their food safety practice at household kitchen
-
To evaluate the impact of individual food safety practice to their food-borne
disease probability
1.2.4 Research question
(1) Do food safety knowledge and perception have impact on individual food safety
practice?
(2) How food safety practice affect to individual food-borne poisoning risk?
1.3 SCOPE OF RESEARCH
The thesis used the data from the survey about Individual Food Poisoning and
Knowledge, Attitude, Practice of household in Ho Chi Minh City (2013). This survey
organized in 24 districts of Ho Chi Minh City from March to April of 2013. The
responders in the investigation were the primary cook at the household while the local
medical staffs were the data collectors.
Although the survey in this theme held annually, the kind of participants is
distinct in every year, vary from the householder (in 2010 and 2013) to the restaurant
worker (in 2012, 2014, 2015, 2016). In addition, the specific responders in the same
kind is different from years, thus the latest data for the household is in 2013 and is not
connected with the 2010 survey so thesis is not able to create the panel data to analyze.
Basing on this secondary data, the scope of research is the behavior and acute
food poisoning statement of the community in Ho Chi Minh City in the period from
March to April of 2013 to evaluate the impact of the factors. Besides the descriptive
statistics, econometric tools are the main methods used in the thesis, such as: factor
analysis, multivariate probit, propensity score matching.
9
1.4 THESIS STRUCTURE
Due to the available of the data, thesis is composed as the structure below:
-
Chapter 1: Introduction about the research problem, the benefit and the scope of
research. This chapter present the general view of FBD and its burden in the world as
well as the outline and objective of the thesis.
-
Chapter 2: Literature review. This chapter review the concept’s definition and
the previous research about the factors and models used in research which are the base
to create the analytic framework and method to analyze the effect of each component.
-
Chapter 3: Research methodology. This chapter provide the framework and
econometric tools which used in the research. In addition, the data source and its
collecting method are presented in this chapter as well as the variables’ description.
-
Chapter 4: Research result. This chapter analyzes the data as well as indicate the
result finding and compare it with other results. The descriptive statistic of variables
are also presented in this chapter
-
Chapter 5: Conclusion and policy implications. This chapter concludes the
research finding, provides implication, further suggestion as well as the research
limitations
10
CHAPTER 2 : LITERATURE REVIEW
2.1 FOOD SAFETY AND FOOD-BORNE DISEASES
According to WHO (2007, p. 11), “Food-borne diseases (FBD) can be defined as
those conditions that are commonly transmitted through ingested food. FBD comprise
a broad group of illnesses caused by enteric pathogens, parasites, chemical
contaminants and biotoxins. Two methodological approaches for food-borne disease
burden estimation exist. Firstly, the etiologic agent (or risk assessment) approach
which commences with the exposure and identifies the exposure levels of agents
commonly transmitted though food, which is followed by determining the proportion
that is food-borne. Secondly, the syndromic (or epidemiological) approach, which
commences with the outcome and estimates incidence of disease syndromes (e.g.
gastroenteritis or chemically induced anaphylaxis), followed by attributing a proportion
to food-borne agents. A comprehensive burden of disease assessment will require a
combination of both approaches”.
WHO (2015, p. X) also estimated there were about 600 million food-borne
illnesses and 420,000 deaths in 2015 due to 31 food-borne hazards, and 40% of the
food-borne disease burden was among children under 5 years of age. However, the
data that is used in the thesis, was collected by interviewing the participants through a
questionnaire and not including any food testing. Therefore, the FBD diagnose was
depended on the responders’ own estimation combine with the assessment of the
medical staff through individual description symptom.
On the other hand, Food safety is “the assurance that food will not cause harm to
human’s health or life” (Vietnam Ministry of Health, 2010). This definition is not as
specific as WHO’s, however it covers the whole procedure of growing, harvesting,
preserving, processing of food instead of only preparing and eating. Due to the wide
11
coverage of Vietnam Ministry of Health and the spreading of Food Safety Regulatory
in Vietnamese population, the thesis used this definition as the concept of Food Safety.
2.2 THE HEALTH BELIEF MODEL:
The HBM was initially derived from the theory of psychology and behavior of
individual (Maiman and Becker, 1974) making decision in uncertainty condition,
where their behavior were predicted by evaluating the “value – expectancy” of possible
outcome. Adapting this theory in health area, the model assumes that individual highly
assesses illness prevention and health status improvement. As a result, they expect their
specific action would prevent disease, improve their health. That expectation is
affected by individual’s calculation about their sensibility to illness, seriousness of
disease as well as the possibility of getting sick by their behavior. According to Glanz
et al (2008, p. 47 - 48), the main components of HBM include:
Table 2.1: The concepts of Health Belief Model
Component
Definition
Application
Perceived susceptibility
Belief about the chances of
Define population(s) at
experiencing a risk or
risk, risk levels.
getting a condition or
Personalize risk based on a
disease
person’s characteristics or
behavior.
Make perceived
susceptibility more
consistent with individual’s
actual risk
Perceived severity
Belief about how serious a
Specify consequences of
condition and its sequelae risks and conditions
are
12
Perceived benefits
Perceived barriers
Belief in efficacy of the
Define action to take: how,
advised action to reduce
where, when; clarify the
risk or seriousness of
positive effects to be
impact
expected
Belief about the tangible
Identify and reduce
and psychological costs of
perceived barriers through
the advised action
reassurance, correction of
misinformation, incentives,
assistance
Cues to action
Strategies to activate
Provide how-to
“readiness”
information, promote
awareness, use appropriate
reminder systems
Self-efficacy
Confidence in one’s ability
Provide training and
to take action
guidance in performing
recommended action.
Use progressive goal
setting.
Give verbal reinforcement.
Demonstrate desired
behaviors.
Reduce anxiety.
These components combine with other individual characteristics then divide into
three groups of factors included: modifying factors, individual belief and action. The
relation, components and impact of each groups showed in the figure below:
13
Modifying factors
Age
Gender
Ethnicity
Personality
Socioeconomics
Knowledge
Individual Beliefs
Perceived
susceptibility
to and severity
of disease
Action
Perceived
threat
Perceived
benefits
Perceived
barriers
Individual
behaviors
Cues to
action
Perceived
self-efficacy
Figure 2.1: Health Belief Model Components and Linkages (Glanz et al, 2008)
Many research implemented HBM in analyzing food safety behavior among
various kind of responders, for instance: restaurant workers (Cho et al, 2010), primary
food preparers in family with young children (Lum, 2013; Meysenburg et al, 2013),
older adults (Hanson and Benedict, 2002). All these papers show that the components
in HBM interact with other, affect on individual’s behavior, especially the food safety
knowledge had strong impact to their perception about food safety.
2.3 EMPIRICAL REVIEWS ON DRIVERS OF FOOD SAFETY PRACTICES:
2.3.1 Socio-economic characteristics
The participants who had college degree or higher degree got a better score in food
safety knowledge and food safety behavior than others (Meysenburg et al, 2013). The
author group used the Health Belief Model with the mixed method analysis to analyze
the sample of 72 participants by script interview and group discussion. Another finding
14
of Unusan (2005) determined a positive effect of education level to the confidence in
food safety practice. Furthermore, higher education level groups get less risk behavior
than the lower ones. However, this research found that socio-economic status does not
correlate with individual food safety practice. In this research, Unusan collected the
data from Turkish households and analyzed using MANOVAs.
On the other hand, Unusan’s research indicated the impact of gender and education
level to the food safety knowledge. The reason for this finding is quite acceptable due
to most of the primary food preparers in household are women, and the high educated
ones likely pay more attention on information. Byrd-Bredbenner et al (2007) and
Mullan et al (2014) found the similar result after reviewing many researches in food
safety issue. Their research also showed that age affect to food knowledge, for instance
the older tend to get higher score in food knowledge. In addition, women would be
more responsible in food safety issue than men (Jevsnik et al, 2006). This consequence
concluded from the investigation of participants by analyzing using ANOVA.
Another research leading by Langiano et al (2012) figured out that the married
participants had more precise food behavior than the singles. Moreover, the more
members the family had, the more accurate practice the primary cook did.
2.3.2 Food safety knowledge
Food preparers mainly study food process knowledge from family’s members and
relatives (Meysenburg et al, 2013). Other research also indicated family as a food
safety knowledge resource which affects individual behavior (Kwon et al, 2008;
Trepka et al, 2006). Kwon investigated participants of the Special Supplemental
Nutrition Program for Woman, Infants, and Children with a questionnaire about food
knowledge and behavior to conclude the result by ANOVA analyzing. Furthermore,
respondents with excellent food knowledge would behave precisely in food practicing
15
(T. H. Vo et al, 2015). These authors group investigated in the canteens’ and
restaurant’s workers by using logistic regression model to get this finding.
However, the finding of Cho et al (2010) show that food safety knowledge of
participants do not influence their food practice. This research focused on restaurant’s
worker with the multiple regression and maximum likelihood estimation. In addition,
Roberts et al (2008) prove that there is only limited distortion in food workers’
behavior even though they have just trained, educated in food safety. Those consolidate
the assumption that knowledge had little impact on individual’s behavior change.
2.3.3 Perception on food safety
The high self-efficiency is confident that they can prevent health threat as well as
FBD when handling food was in their control (Meysenburg et al, 2013). This
confidence would decrease whether the food were prepared by others. In addition, ones
had suffer food-borne illness or caused the illness for family member due to their
improper handling food also were less confident in their food prepare.
Many studies have shown mixed results on food safety perception and behavior.
Nesbitt et al (2013) found that many consumers felt that food contamination occurs
before food reaches their kitchen and majority of those who experienced FBD felt that
their illness was cause by food prepared outside the home. However, Unusan’s
research (2007) indicated that consumer did not recognize food poisoning/FBD as a
health problem, they even acknowledged it as a normal issue. This misleading
awareness leads to the fact that they rarely tend to adjust food safety behavior or pay
attention on food safety issue.
Jevsnik et al (2006) found the fact that the household cook preferred farmer’s
product to the industrial factories. They believed that the food produced by farmer
would be safer. However, the consumers said that they were not responsible for food
safety but claim this is food handler (farmer, food factory, retailing, catering) and the