Ebook Principles and practice of mechanical ventilation (3/E): Part 2
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (17.82 MB, 760 trang )
IX
PHYSIOLOGIC
EFFECT OF
MECHANICAL
VENTILATION
This page intentionally left blank
EFFECTS OF MECHANICAL
VENTILATION ON CONTROL
OF BREATHING
35
Dimitris Georgopoulos
PHYSIOLOGY
EFFECTS OF MECHANICAL
VENTILATION ON FEEDBACK SYSTEMS
Chemical Feedback
Response of Respiratory Motor Output to Chemical Stimuli
Operation of Chemical Feedback
Neuromechanical Feedback
Neuromechanical Inhibition
Behavioral Feedback
The main reasons for instituting mechanical ventilation are
to decrease the work of breathing, support gas exchange,
and buy time for other interventions to reverse the cause of
respiratory failure.1 Mechanical ventilation can be applied in
patients who are making or not making respiratory efforts,
whereby assisted or controlled modes of support are used,
respectively.1 In patients without respiratory efforts, the
respiratory system represents a passive structure, and thus
the ventilator is the only system that controls breathing.
During assisted modes of ventilator support, the patient’s
system of control of breathing is under the influence of the
ventilator pump.2–4 In the latter instance, ventilatory output
is the final expression of the interaction between the ventilator and the patient’s system of control of breathing. Thus,
physicians who deal with ventilated patients should know
the effects of mechanical ventilation on control of breathing,
as well as their interaction. Ignorance of these issues may
prevent the ventilator from achieving its goals and also lead
to significant patient harm.
PHYSIOLOGY
The respiratory control system consists of a motor arm,
which executes the act of breathing, a control center located
in the medulla, and a number of mechanisms that convey
information to the control center.5,6 Based on information, the control center activates spinal motor neurons that
INTERACTIVE EFFECTS OF
PATIENT-RELATED FACTORS AND
VENTILATOR ON CONTROL OF BREATHING
Mechanics of Respiratory System
Characteristics of Muscle Pressure Waveform
FUTURE
CONCLUSION
subserve the respiratory muscles (inspiratory and expiratory); the intensity and rate of activity vary substantially
between breaths and between individuals. The activity of
spinal motor neurons is conveyed, via peripheral nerves, to
respiratory muscles, which contract and generate pressure
(Pmus). According to equation of motion, Pmus at time t
during a breath is dissipated in overcoming the resistance
(Rrs) and elastance (Ers) of the respiratory system (inertia is
assumed to be negligible) as follows:
˙ + Ers × ΔV(t)
Pmus(t) = Rrs × V(t)
(1)
where ΔV(t) is instantaneous volume relative to passive
functional residual capacity and V˙ (t) is instantaneous flow.
Equation (1) determines the volume–time profile and,
depending on the frequency of respiratory muscle activation, ventilation. Volume–time profile affects Pmus via neuromechanical feedback; inputs generated from other sources
(cortical inputs) may modify the function of control center.
Ventilation, gas-exchange properties of the lung, and cardiac
function determine arterial blood gases, termed arterial oxygen tension (PaO 2) and arterial carbon dioxide tension (Pa CO2),
which, in turn, affect the activity of control center via peripheral and central chemoreceptors (chemical feedback). This
system can be influenced at any level by diseases or therapeutic interventions.
During mechanical ventilation, the pressure provided
by the ventilator (Paw) is incorporated into the system.3
Thus, the total pressure applied to respiratory system at
805
806
Part IX
Physiologic Effect of Mechanical Ventilation
Ventilator factors
Triggering
Control
Variables
Cycling off
Patient factors
RS mechanics
Pmus waveform
Response of
ventilator to Pmus
.
Pmus(t) + Paw(t) = V (t) · Rrs + ΔV(t ) · Ers
Volume–time profile
Response of Pmus
to ventilator-delivered
breath
Chemical – Neuromechanical – Behavioral
Feedback
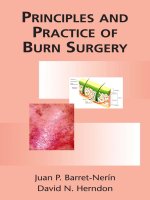
FIGURE 35-1 Schematic of variables that determine the volume–time profile during mechanical ventilation. Neuromechanical, chemical, and behavioral feedback systems are the main determinants of Pmus. The functional operation of the ventilator mode (triggering, control, and cycling-off variables) and patient-related factors (namely, respiratory system mechanics and the Pmus waveform) determine the response of the ventilator to Pmus.
ΔV(t), instantaneous volume relative to passive functional residual capacity of respiratory system; Ers, elastance of the respiratory system; Paw(t),
˙
airway (ventilator) pressure; Pmus(t), instantaneous respiratory muscle pressure; Rrs, resistance of the respiratory system; RS, respiratory system; V
(t), instantaneous flow.
time t [PTOT(t)] is the sum of Pmus(t) and Paw(t). As a result,
the equation of motion is modified as follows:
PTOT(t) = Pmus(t) + Paw(t)
˙ × Rrs + ΔV(t) × Ers
= V(t)
(2)
The relationships of Equation (2) determine the volume–
time profile during mechanical ventilation, which via neuromechanical, chemical, and behavioral feedback systems
affects the Pmus waveform (Fig. 35-1). The ventilator pressure, by changing flow and volume, may influence these
feedback systems and thus alter either the patient’s control of
breathing itself or its expression. In addition, Pmus, depending on several factors, alters the Paw waveform (Fig. 35-1).
Thus, during assisted mechanical ventilation (i.e., Pmus ≠ 0),
ventilatory output is not under the exclusive influence of
patient’s control of breathing; instead, it represents the final
expression of an interaction between ventilator-delivered
pressure and patient respiratory effort.
EFFECTS OF MECHANICAL
VENTILATION ON FEEDBACK SYSTEMS
Chemical Feedback
Chemical feedback refers to the response of Pmus to PaO 2,
Pa CO2, and pH.5–7 In spontaneously breathing and mechanically ventilated patients, this system is an important determinant of respiratory motor output both during wakefulness
and sleep.7–11
Mechanical ventilation can influence chemical feedback
simply by altering the three variables PaO 2, Pa CO2, and pH.
Hypoxemia, hypercapnia, or acidemia may be corrected
by mechanical ventilation and thus modify activity of the
medullary respiratory controller via peripheral and central
chemoreceptors.5,12 The effects of mechanical ventilation on
gas-exchange properties of the lung are beyond the scope of
this chapter and are discussed in Chapter 37. In this chapter, the fundamental elements of the response of respiratory
motor output to chemical stimuli, their relationship to unstable breathing, and the operation of chemical feedback during
mechanical ventilation are reviewed.
Response of Respiratory Motor
Output to Chemical Stimuli
CARBON DIOXIDE STIMULUS
Carbon dioxide (CO2) is a powerful stimulus of breathing.5,12
This stimulus, expressed by Pa CO2, largely depends on the
product of tidal volume (VT) and breathing frequency ( f )
(i.e., minute ventilation) according to Equation (3):
˙CO /[V × f(1 − V /V )]
Pa CO2 = 0.863 V
T
D
T
2
(3)
where VCO2 is CO2 production, and VD/VT is the deadspace-to-tidal-volume ratio. Because minute ventilation is
an adjustable variable in ventilated patients, understanding
the relationship between respiratory motor output and CO2
stimuli is of fundamental importance.
Chapter 35
807
sleep; propensity increases as CO2 reserve decreases. Similar
to wakefulness, the response of respiratory motor output to
CO2 is mediated mainly by the intensity of respiratory effort,
whereas respiratory rate decreases abruptly to zero (apnea)
when the CO2 apneic threshold is reached.19
350
300
% of baseline
Effects of Mechanical Ventilation on Control of Breathing
250
200
150
100
OTHER CHEMICAL STIMULI
50
0
20
25
30
40
35
PETCO2 (mm Hg)
45
50
55
FIGURE 35-2 Schematic of the response of respiratory frequency
(open squares) and pressure-time product of the inspiratory muscles
per breath (an index of the intensity of patient effort, closed squares),
both expressed as a percentage of values during spontaneous eupnea
(baseline), to CO2 challenge in conscious healthy subjects ventilated
with a high level of ventilator assistance. PETCO2 is end-tidal PCO2, and
the dotted vertical line is PETCO2 during spontaneous breathing (eupnea). Contrast the vigorous response of intensity of inspiratory effort
to CO2, even in the hypocapnic range, with the response of respiratory
frequency, which remains at eucapnic level over a broad range of CO2
stimuli. The response is based on data from references 7 and 13 to 16.
Several studies have examined the respiratory motor output to CO2 in ventilated, conscious, healthy subjects.7,13–16
Major findings include
1. Manipulation of Pa CO2 over a wide range has no appreciable effect on respiratory rate. Despite hypocapnia, subjects
continue to trigger the ventilator with a rate similar to
that of eucapnia. Respiratory rate increases slightly when
Pa CO2 approaches values well above eucapnia (Fig. 35-2).
2. The intensity of respiratory effort (respiratory drive)
increases progressively as a function of PCO2. This response
is evident even in hypocapnic range. The response slope
increases progressively with increasing CO2 stimuli,
reaching its maximum in the vicinity of eucapnic values
(see Fig. 35-2).
3. There is no fundamental difference in the response to
CO2 between various ventilator modes.
4. Above eupnea, the slope of the response does not differ significantly with that observed during spontaneous
breathing, suggesting that mechanical ventilation per se
does not considerably modify the sensitivity of respiratory system to CO2.
During sleep (or sedation), the response of respiratory
motor output to CO2 differs substantially from that during wakefulness, secondary to loss of the suprapontine
neural input to the medullary respiratory controller.10,17 In
ventilated sleeping subjects, a decrease in Pa CO2 by a few
millimeters of mercury causes apnea.10 Respiratory rhythm
is not restored until Pa CO2 has increased significantly above
eupneic levels. The difference between eupneic Pa CO2 and
Pa CO2 at apneic threshold, referred to as CO2 reserve,18
depends on several factors (see Response of Respiratory
Motor Output to Chemical Stimuli—Chemical stimuli and
unstable breathing). This reserve determines the propensity of an individual to develop breathing instability during
The effects of mechanical ventilation on the response of
respiratory motor output to stimuli other than CO2 have not
been studied adequately. In a steady state during wakefulness, the effects of oxygen (O2) and pH on breathing pattern are similar qualitatively to that observed with CO2:
Changes in O2 and pH mainly alter the intensity of patient
effort, whereas respiratory rate is affected considerably
less.5,12 There is no reason to expect a different response pattern during mechanical ventilation. Indeed, this is the case
regarding the hypoxic response in normal conscious subjects
ventilated in assist-control mode during eucapnia.20 Indirect
data also revealed that during eucapnia, the sensitivity of
respiratory motor output to hypoxia was not modified by
mechanical ventilation.20 During mild hypocapnia, however,
the response was attenuated, whereas at moderate hypocapnia (end-tidal PCO2 approximately 31 mm Hg) the response
was negligible. The latter observations may be relevant clinically because ventilated patients do not always keep Pa CO2 at
eucapnic levels and can become hypocapnic.16
CHEMICAL STIMULI AND UNSTABLE BREATHING
The response pattern of respiratory motor output to CO2
during sleep is relevant to the occurrence of periodic
breathing in mechanically ventilated patients. Studies indicate that this breathing pattern might increase the morbidity and mortality of critically ill patients because it can
cause sleep fragmentation and patient–ventilator dyssynchrony.21–23 Sleep deprivation may cause serious cardiorespiratory,24,25 neurologic,26,27 immunologic, and metabolic
consequences.28–31
The following is a brief review of the factors that can lead
to unstable breathing. In a closed system governed mainly
by chemical control (such as occurs during sleep or sedation), a transient change in ventilation at a given metabolic
rate (ΔV˙ initial) will result in a transient change in alveolar gas
tensions. This change is sensed by peripheral and central
chemoreceptors, which, after a variable delay, exert a corrective ventilatory response (ΔV˙ corrective) that is in the opposite
direction to the initial perturbation32,33 (Fig. 35-3). The ratio
of ΔV˙ corrective to ΔV˙ initial defines the loop gain of the system.32
Loop gain is a dimensionless index that is the mathematical product of three types of gains: plant gain (the relationship between the change in gas tensions in mixed pulmonary
capillary blood and ΔV˙ initial), feedback gain (the relationship
between gas tensions at the chemoreceptor level and those
at the mixed pulmonary capillary level), and controller gain
(the relationship between ΔV˙ corrective and the change in gas
tensions at the chemoreceptor level) (Fig. 35-3). Loop gain
has both a magnitude and a dynamic component.32,33 In this
808
Part IX
Physiologic Effect of Mechanical Ventilation
Gplant
TABLE 35-1: EFFECTS OF MECHANICAL
VENTILATION ON GAIN FACTORS
AND GAIN CHANGES
FRC ↑
. .
V/Q ↓ ↔ ↑
VD/VT ↓ ↔ ↑
PaCO2 ↓ ↔ ↑
CO ↓ ↔ ↑
Metabolic rate ↓ ↔ ↑
.
ΔVinitial
ΔPCCO2, ΔPCO2
Gfeedback
Mixing ↓ ↔ ↑
Circulatory delay ↓ ↔ ↑
. Loop Gain.
(ΔVcorrective /ΔVinitial)
.
ΔVcorrective
Diffusion delay ↔
ΔPchCO2, ΔPchO2
Gcontroller
Chemosensitivity ↔
Pmus ↓ ↔ ↑
Ers ↓ ↔ ↑
Rrs ↓ ↔ ↑
Paw ↑
FIGURE 35-3 Schematic of the variables that determine the propensity
of an individual to develop periodic breathing in a closed system dominated by chemical feedback. Loop gain is the product of three gains:
˙
(the
plant, feedback, and controller. Instability occurs when ΔV
corrective
˙
(the
transient
final response) is 180 degrees out of phase with ΔV
initial
˙
˙
/ΔV
is greater than 1. Mechanical
initial perturbation) and ΔV
corrective
initial
ventilation, by affecting almost all variables of the system (↑, increase;
↔, no change; ↓, decrease), may change both the magnitude and the
dynamic component of loop gain and thus the propensity of an individual to develop periodic breathing. CO, cardiac output; ΔPCCO2
and ΔPCO2, the difference in partial pressures of CO2 and O2 in mixed
pulmonary capillary blood, respectively; ΔPchCO2 and ΔPchO2, the difference in partial pressure of CO2 and O2 at chemoreceptors (peripheral and central), respectively; Ers and Rrs, elastance and resistance of
respiratory system, respectively; FRC, functional residual capacity; LG,
Gplant, Gfeedback, and Gcontroller, loop, plant, feedback, and controller gains,
respectively; PaCO 2 alveolar partial pressure of CO2; Paw, airway (ventilator) pressure; Pmus, pressure developed by respiratory muscles; V Q,
ventilation–perfusion ratio; VD/VT, dead-space fraction.
system, instability occurs when the corrective response is
180 degrees out of phase with initial disturbance (dynamic
component) and loop gain is greater than 1 (magnitude
component). This instability leads to fluctuation in chemical
stimuli, namely, PCO2. If PCO2 reaches the apneic threshold,
apnea occurs.
Positive-pressure breathing exerts multiple effects on
loop gain by influencing almost all the factors that determine
plant, feedback, and controller gains. The effects are complex and at times opposing and variable (Table 35-1; see also
Fig. 35-3). Nevertheless, the effect of mechanical ventilation
on controller gain exerts the most powerful influence on the
propensity to develop breathing instability.8,19,21,23 The magnitude and direction of the change in controller gain depends
on the ventilator mode, the level of assistance, the mechanics
Gain Factors (Influence)
Ventilator
Effect*
Lung volume (stabilizing)
↑
↓Gplant
Cardiac output (destabilizing)
↓
↑Gplant, ↑Gfeedback
Thoracic blood volume
(destabilizing)
Paw response to Pmus
(destabilizing)
Alveolar PCO2 (stabilizing)
↓
↑Gfeedback
↑
↑Gcontroller
↓
↓Gplant
Alveolar PO2 (stabilizing)
↑
↓Gplant, ↓Gcontroller
Respiratory elastance
(destabilizing)
↓
↑Gcontroller
Gain Change
Abbreviations: ↓, decrease; ↑, increase; Paw, airway pressure; Pmus, respiratory
muscle pressure.
*Mechanical ventilation may also exert opposite effects on the various gain factors.
of the respiratory system, and the Pmus waveform (see the
section Interactive Effects of Patient-Related Factors and
Ventilator on Control of Breathing).8,16,19,21 Disease states as
well as medications (e.g., sedatives) also may interfere with
the effects of mechanical ventilation on loop gain. For example, positive-pressure ventilation may increase or decrease
cardiac output, causing corresponding changes in circulatory delay depending on cardiac function and intravascular
volume (see Chapter 36).34–37 It has been shown that nocturnal mechanical ventilation in patients with congestive heart
failure decreases the frequency of Cheyne-Stokes breathing,
presumably by causing an increase in cardiac output secondary to afterload reduction.38–40 Sedatives at moderate doses,
commonly used in ventilated patients, decrease considerably the loop gain, partly mitigating the effect of mechanical
ventilation on controller gain and thus promote ventilatory
stability.41
In addition to CO2, O2 and pH can play a key role in
producing unstable breathing in ventilated patients during
sleep (or sedation). It is well known that hypoxia, acting via
peripheral chemoreceptor stimulation, decreases Pa CO2. The
result reduces the plant gain (stabilizing influence); for a
given change in alveolar ventilation, Pa CO2 will change less
when baseline Pa CO2 is low than when it is high.18 Hypoxia,
however, increases the controller gain to a much greater
extent42 because the slope of ventilatory response to CO2
below eupnea increases,12 a highly destabilizing influence.32,33
Similar principles apply if pH is considered as a chemical
stimulus; acidemia decreases the plant gain (lowers Pa CO2)
and increases, to a much lesser extent, the controller gain.18,42
During mechanical ventilation, the propensity to unstable
breathing in the face of changing O2 and pH stimuli depends
on a complex interaction between the effects of these stimuli
and mechanical ventilation on plant, feedback, and controller gains (Fig. 35-4; see also Table 35-1).
Chapter 35
Effects of Mechanical Ventilation on Control of Breathing
809
Metabolic acidosis
1
VT (I)
0
Pm
10
(cm H2O) 0
Edi
(a.u.)
40
CO2 reserve = –7.1 mm Hg
PETCO2
(mm Hg)
0
A
1 min.
Metabolic alkalosis
1
VT (I)
0
Pm
(cm H2O) 10
∫Edi
(a.u.)
CO2 reserve = –3.4 mm Hg
40
PETCO2
(mm Hg)
0
B
1 min.
Hypoxia
1
VT (I)
0
Pm
10
(cm H2O) 0
Edi
(a.u.)
40
CO2 reserve = –3.4 mm Hg
PETCO2
(mm Hg)
0
C
1 min.
FIGURE 35-4 Tidal volume (VT), airway
pressure (Pm), integrated diaphragmatic
electrical activity (Edi, arbitrary units), and
partial pressure of end-tidal CO2 (PETCO2)
in a tracheostomized dog during non–rapid
eye movement sleep without and with
pressure-support ventilation at a pressure
level that caused periodic breathing. (A) At
a background of 5 hours of metabolic acidosis (pH 7.34, HCO3− 16 mEq/L, Pa CO2
30 mm Hg). (B) At a background of 1 hour
of metabolic alkalosis (pH 7.51, HCO3−
35 mEq/L, Pa CO2 44 mm Hg). (C) During
hypoxia (PaO2 47 mm Hg, Pa CO2 31 mm Hg).
At a background of metabolic acidosis, CO2
reserve was quite high; consequently, the
pressure level that caused periodic breathing
(20 cm H2O) was significantly higher than
the corresponding values (approximately
10 cm H2O) during metabolic alkalosis or
hypoxia. Hyperventilation during spontaneous breathing was similar during metabolic
acidosis and hypoxia (similar stabilization
influence via a decrease in plant gain secondary to low Pa CO2), indicating that the destabilizing influence of hypoxia was caused
by an increase in controller gain (hypoxic
increase in the slope of CO2 below eupnoea).
(Used, with permission, from Dempsey et al.
J Physiol. 2004;560:1–11, based on data from
Nakayama H, Smith CA, Rodman JR, et al.
Effect of ventilatory drive on carbon dioxide
sensitivity below eupnea during sleep. Am J
Respir Crit Care Med. 2002;165:1251–1260.)
810
Part IX
Physiologic Effect of Mechanical Ventilation
Operation of Chemical Feedback
PET CO2
(mm Hg)
20
Flow
–1
(L s )
70
Paw
(cm H2O)
The ventilator mode is a major determinant of driving
pressure for flow and thus arterial blood gases. Before discussing the operation of chemical feedback, it is useful to
review briefly the functional features of three main modes
of assisted ventilation, namely, assist-control ventilation
(ACV), pressure-support ventilation (PSV), and proportional-assist ventilation (PAV) (for detailed descriptions,
see Chapters 6, 8, and 12). Figure 35-5 shows the response
of the ventilator to respiratory effort in a representative
subject ventilated with each mode in the presence and
absence of CO2 challenge.16 With CO2 challenge, Paw
decreases with ACV, it remains constant with PSV, and it
increases with PAV. Pressure-time product of inspiratory
muscle pressure (PTP-PmusI) is an accurate index of the
intensity of inspiratory effort.43 With ACV, the ratio of
V T to PTP-PmusI per breath (neuroventilatory coupling)
decreases with increasing Pmus; the ratio is largely independent of inspiratory effort with PAV. With PSV, V T/
PTP-PmusI per breath may change in either direction with
increasing Pmus, depending on factors such as the level of
pressure assist and cycling-off criterion, change in Pmus,
and mechanics of the respiratory system. With PSV, in the
absence of active termination of pressure delivery (with
expiratory muscle contraction), the ventilator delivers a
minimum V T , which may be quite high, depending on the
pressure level, mechanics of the respiratory system, and
cycling-off criterion.19
Assume that in a ventilated patient Pa CO2 drops because
of an increase in the set level of assistance or decrease in
metabolic rate and/or VD/VT ratio.44 During wakefulness,
patients will react to this drop by decreasing the intensity of their inspiratory effort, whereas the breathing frequency will remain relatively constant (see “Response of
Respiratory Motor Output to Chemical Stimuli,” above).
The extent to which a patient is able to prevent respiratory alkalosis via operation of chemical feedback depends
almost exclusively on the relationship between the intensity
of patient inspiratory effort and the volume delivered by the
ventilator (i.e., VT/PTP-PmusI). Similarly, if Pa CO2 increases
(decrease in assistance level, increase in metabolic rate
and/or VD/VT ratio), the patient will increase the intensity
of inspiratory effort and, to much lesser extent, respiratory
frequency. Thus, VT/PTP-PmusI per breath is critical for
the effectiveness of chemical feedback to compensate for
changes in chemical stimuli (Pa CO2). For given respiratory
system mechanics, VT/PTP-PmusI is heavily dependent on
the mode of support. Thus, the effectiveness of chemical
feedback in compensating for changes in chemical stimuli
should be mode-dependent. Modes of support that permit
the intensity of patient inspiratory effort to be expressed
on ventilator-delivered volume improve the effectiveness of
chemical feedback in regulating Pa CO2 and particularly in
35
0
10
0
2
0
Pes
(cm H2O)
Volume
(L)
–2
2
0
–2
10
0
–10
–20
A
B
5s
C
D
5s
E
F
5s
FIGURE 35-5 End-tidal carbon dioxide tension (PETCO2), airway pressure (Paw), flow (inspiration up), volume (inspiration up), and esophageal (Pes)
pressure in a representative subject during proportional-assist ventilation (A, B), pressure-support ventilation (C, D), and volume-control ventilation
(E, F) in the absence (A, C, E) and presence (B, D, F) of CO2 challenge. With CO2 challenge, Paw decreases with assist-control ventilation (the ventilator antagonizes patient’s effort); it remains constant with pressure-support ventilation (no relationship between patient effort and level of assist); and
it increases with proportional-assist ventilation (positive relationship between effort and pressure assist). (Used, with permission from Mitrouska J,
Xirouchaki N, Patakas D, et al. Effects of chemical feedback on respiratory motor and ventilatory output during different modes of assisted mechanical
ventilation. Eur Respir J. 1999;13:873–882.)
Chapter 35
0.8
VT/PTP-PmusI
(L/cm H2O/s)
+
0.6
+
0.4
*
0.2
*
0
PAV
PS
AVC
FIGURE 35-6 Ratio (mean ± SD) of tidal volume to pressure–time
product of inspiratory muscles (VT/PTP-PmusI) in normal, conscious
subjects ventilated with three modes of assisted ventilation in the
absence and presence of CO2 challenge (inspired CO2 concentration
increased in small steps until intolerance developed). Open and closed
bars represent zero and final (highest) concentration of inspired CO2,
respectively. AVC, assist-volume control; PAV, proportional-assist ventilation; PS, pressure-support ventilation. Asterisk indicates significant
difference from the value without CO2 challenge. Plus sign indicates
significant difference from the corresponding value with PAV. With
each mode, subjects were ventilated at the highest comfortable level of
assistance (corresponding to 80% reduction of patient resistance and
elastance with PAV, 10 cm H2O of pressure support, and 1.2-L tidal
volume with AVC). With CO2 challenge, VT/PTP-PmusI, decreased
significantly when the subjects were ventilated with PS and AVC,
but it remained relatively constant with PAV. Without CO2 challenge,
VT/PTP-PmusI was significantly higher with PS and AVC than with
PAV. This response pattern caused severe respiratory alkalosis with PS
and AVC (PETCO2 decreased to approximately 22 mm Hg with both
modes) but not with PAV (PETCO2 approximately 30 mm Hg). Unlike
with PS and PAV, subjects ventilated with AVC could not tolerate high
values of PETCO2 (final PETCO2 was approximately 7, 11, and 13 mm
Hg higher than baseline eupnea, respectively, with AVC, PS, and PAV).
(Based on data from Mitrouska et al.16)
preventing respiratory alkalosis. In normal conscious subjects receiving maximum assistance on the three main ventilator modes,16 the ability of the subject to regulate Pa CO2
depends on the operational principles of each mode, specifically in terms of VT/PTP-PmusI (Fig. 35-6). At all levels of
CO2 stimulation, preservation of neuroventilatory coupling
increased progressively from ACV to PSV to PAV; the ability of subjects to regulate Pa CO2 followed the same pattern.16
Neurally adjusted ventilatory assist (NAVA) is a new mode
of support that, similar to PAV, uses patient effort to drive
the ventilator.45–47 The electrical activity of the diaphragm
is obtained with a special designed esophageal catheter and
serves as a signal to link inspiratory effort to ventilator pressure (see Chapter 13). Because neuroventilatory coupling
is preserved, the principles described above also apply to
NAVA.46,47
During sleep or sedation, the tendency to develop hypocapnia with ACV and PSV (see Chapter 57 for the effects
of mechanical ventilation on sleep) may have serious consequences because a drop of a few millimeters of mercury
in Pa CO2 leads to apnea and periodic breathing.8,19 Thus,
excessive assistance with ACV and PSV promotes unstable
breathing secondary to impaired neuroventilatory coupling;
Effects of Mechanical Ventilation on Control of Breathing
811
controller gain remains high in the face of low inspiratory
effort (Fig. 35-7). Unstable breathing, however, during sleep
secondary to mechanical ventilation may be prevented or
attenuated with PAV and NAVA that does not guarantee a
minimum VT .8,19,46,47 Modes that decrease the volume delivered by a ventilator in response to any reduction in the
intensity of patient effort enhance breathing stability and
may be associated with better sleep quality.48 Nevertheless, if
the assist setting during PAV or NAVA is such that controller gain increases considerably, and the inherent loop gain
of the patient is relatively high, the patient will be at risk of
developing unstable breathing.23,33,41,49,50
These principles may be altered by disease states and
therapeutic interventions. Although little is known about
the interaction between disease states and mechanical
ventilation on control of breathing, two examples help
in illustrating the point. First, in conscious patients with
sleep apnea syndrome, a drop in Pa CO2 because of brief
(40 seconds) hypoxic hyperventilation resulted, contrary to
healthy subjects, in significant hypoventilation and triggering of periodic breathing in some patients.51 This hypoventilation was interpreted as evidence of a defect (or reduced
effectiveness) of short-term poststimulus potentiation, a
brainstem mechanism that promotes ventilatory stability.51 In this situation, a level of assistance that causes a significant decrease in Pa CO2 may promote unstable breathing
in awake patients with sleep apnea syndrome, a situation
closely resembling that observed during sleep. Second,
studies in ventilated critically ill patients have shown that
when awake patients are unable to increase VT appropriately as a result of the mode used (i.e., PSV), they increase
respiratory rate in response to a chemical challenge.52
Behavioral feedback, however, may underlie this response
pattern. In sedated patients with acute respiratory distress
syndrome (in whom behavioral feedback is not an issue)
receiving PSV, considerable variation in Pa CO2 elicited a
steady-state response limited to the intensity of breathing
effort, a response pattern similar to that observed in normal subjects.9,16
Neuromechanical Feedback
INTRINSIC PROPERTIES
OF RESPIRATORY MUSCLES
For a given neural output, Pmus decreases with increasing
lung volume and flow, as dictated by the force-length and
force-velocity relationships of inspiratory muscles, respectively.53 Therefore, for a given level of muscle activation,
Pmus should be smaller during mechanical ventilation than
during spontaneous breathing if pressure provided by the
ventilator results in greater flow and volume. It has been
shown in healthy subjects ventilated with PSV that, compared with spontaneous breathing, the relationship between
electrical activity (Edi) and pressure-time product of diaphragm (PTPdi) is shifted to the left; thus, at any given level
of Edi, PTPdi is reduced.54
812
Part IX
Physiologic Effect of Mechanical Ventilation
Chin EMG
C3/A2
C4/A1
EOG(R)
EOG(L)
Rib cage
Abdomen
Volume
Flow
PETCO2
Paw
A
B
C
Chin EMG
C3/A2
C4/A1
EOG(R)
EOG(L)
Rib cage
Abdomen
Volume
Flow
PETCO2
Paw D
30 s
FIGURE 35-7 Polygraph tracings in a healthy subject during non-rapid eye movement sleep with and without pressure-support ventilation.
(A) Spontaneous breathing with continuous positive airway pressure (CPAP). (B) to (D) Pressure support of 3, 6, and 8 cm H2O, respectively. Periodic
breathing with central apneas developed with pressure support of 8 cm H2O. C3/A2 and C4/A1, electroencephalogram channels; EMG, electromyogram; EOG, electrooculogram (right [R] and left [L]); Paw, airway pressure; PETCO2, end-tidal PCO2. (Used, with permission, from Meza, et al.
Susceptibility to periodic breathing with assisted ventilation during sleep in normal subjects. J Appl Physiol. 2003;167:1193–1199.)
The influence and consequences of mechanical feedback
during mechanical ventilation have not been studied satisfactorily. It is possible that this type of feedback is of clinical
significance in patients with dynamic hyperinflation (high
end-expiratory lung volume), high ventilatory requirements
(requirements for high flow and volume), and/or impaired
neuromuscular capacity.
REFLEX FEEDBACK
The characteristics of each breath are influenced by various reflexes that are related to lung volume or flow and
mediated, after a latency of a few milliseconds, by receptors located in the respiratory tract, lung, and chest wall.5,6
Mechanical ventilation may stimulate these receptors
by changing flow and volume. In addition, changes in
Chapter 35
0.6
0.4
ΔTen (s)
0.2
–0.4 –0.3
0
–0.2 –0.1
–0.2
0.1
0.2
0.3
0.4
0.5
–0.4
–0.6
ΔText (s)
y = –0.004 + 0.897x, P < 0.001
FIGURE 35-8 Relationship between the changes in the time that
mechanical inspiration extended into neural expiration (ΔText, expiratory asynchrony) and neural expiratory time (ΔTen) in mechanically
ventilated patients with acute respiratory distress syndrome. Closed
circles, open circles, and open triangles represent ΔText induced by
changes in volume (at constant flow), flow (at constant volume), and
pressure support, respectively. Solid line, regression line. (Based on data
from Kondili E, Prinianakis G, Anastasaki M, Georgopoulos D. Acute
effects of ventilator settings on respiratory motor output in patients
with acute lung injury. Intensive Care Med. 2001;27:1147–1157.)
ventilator settings, inevitably associated with changes in
volume and flow, also may elicit acute Pmus responses
mediated by reflex feedback. In sedated patients with acute
respiratory distress syndrome, manipulation of ventilator
settings altered immediately (within one breath) the neural respiratory timing, whereas respiratory drive remained
constant.9,55 Specifically, decreases in V T and pressure support and increases in inspiratory flow caused an increase in
respiratory frequency. Depending on the type of alteration,
changes in respiratory frequency were mediated via alteration in neural inspiratory and expiratory time; increases in
inspiratory flow caused increases in respiratory frequency
mainly by decreasing neural inspiratory time; decreases in
V T and pressure support caused increases in respiratory
frequency by decreasing neural expiratory time. This reflex
response was similar, at least qualitatively, to that observed
in healthy subjects during wakefulness and sleep.56–60 There
was a strong dependency of neural expiratory time on the
time that mechanical inflation extended into neural expiration; neural expiratory time increased proportionally to
the increase in the delay between the ventilator cycling off
and the end of neural inspiratory time (Fig. 35-8).9,55 This
finding indicates that expiratory asynchrony may elicit a
reflex timing response. A subsequent study in a general
intensive care unit population confirmed the dependency
of neural expiratory time on expiratory asynchrony.61 The
most likely explanation for the timing response is the
Herring-Breuer reflex.
The final response may be unpredictable depending on
the magnitude and type of lung volume change, the level
of consciousness, and the relative strength of the reflexes
involved. Nevertheless, reflex feedback should be taken
Effects of Mechanical Ventilation on Control of Breathing
813
into account when ventilator strategies are planned. A few
examples may help in illustrating the importance of reflex
feedback in patient–ventilator interaction. Assume that the
patient is receiving pressure support that is being decreased
during weaning. This results in lower VT , which through
reflex feedback decreases neural expiratory time, causing
an increase in respiratory frequency.9,55 This increase should
not be interpreted as patient intolerance to the decrease in
pressure support. Consider another patient with obstructive
lung disease receiving ACV. VT is decreased at a constant
inspiratory flow so as to reduce the magnitude of dynamic
hyperinflation (less volume is exhaled over a longer period).
The lower VT usually results in less delay in breath termination as compared with the end of neural inspiration, which
through vagal feedback will decrease neural expiratory
time, limiting the effectiveness of this strategy for reducing
dynamic hyperinflation.55 Assume in another patient receiving ACV that inspiratory flow is increased at a constant VT ,
with the intent of reducing inflation time and providing
more time for expiration so as to reduce dynamic hyperinflation. This step causes a reflex decrease in neural inspiratory
time and an increase in respiratory frequency. Mechanical
expiratory time may change in either direction depending mainly on the relation between neural and mechanical
inspiratory time. In patients receiving ACV, expiratory time
showed a variable response to changes in flow rate; some
patients actually demonstrate a reduced expiratory time
with a higher flow,62 which cancels the desired reduction in
dynamic hyperinflation.
There are neural reflexes that inhibit inspiratory muscle
activity if lung distension exceeds a certain threshold, which
is well below total lung capacity (Hering-Breuer reflex).6,63,64
These reflexes protect the lung from overdistension, which is
associated with lung injury.65,66 Pressure-control or volumecontrol modes of assisted ventilation considerable interfere
with the ability of these reflexes to regulate tidal volume.16,67
With these modes, as a result of neuroventilatory uncoupling
(high VT/PTP-PmusI), overassistance may result in high tidal
volume leading to regional or global lung overdistension.
Conversely, recent evidence indicates that ventilator modes
that permit reflex feedback to regulate the tidal volume and
respiratory rate (viz., NAVA, PAV) may protect against or
lessen ventilator-induced lung injury.
Brander et al68 randomized anesthetized rabbits with early
experimental acute lung injury into three ventilator strategies: NAVA (nonparalyzed), volume control with tidal volume of 6 mL/kg (paralyzed, protective strategy), and volume
control with tidal volume of 5 mL/kg (paralyzed, injurious
strategy). Animals randomized to NAVA selected an average
tidal volume of 2.7 ± 0.9 mL/kg and respiratory rate up to
three times higher than that in both controlled ventilation
groups—a breathing-pattern response that can be explained
by vagally controlled reflexes.6,63,64 Compared to the 15 mL/
kg group, animals ventilated with either NAVA or volume
control at 6 mL/kg exhibited less ventilator-induced lung
injury, as indicated by lung injury scores, lung wet-to-dry
ratio, and lung and systemic biomarkers (Fig. 35-9). These
600
Physiologic Effect of Mechanical Ventilation
VC 15 mL/kg
VC 6 mL/kg
NAVA
PaO to FIO2 ratio
2
p (l-g) = < 0.001
400
12
†,‡
§
200
p = 0.028
8
0 0.5 1
A
1800
2
3
4
IL-8 concentration in BAL fluid and lungs
Lung
BAL
tissue
fluid
B
90000
160
‡
30000
600
‡
¶
0
C
45000
¶ ¶ ¶
¶ ¶ ¶
dependent right nondependent
right lower lobe
lower lobe
pg/mL
pg/mL
§
§
pg/g protein
60000
¶
¶
nondependent
right lower lobe
Tissue
factor
PAI-l
6
‡
§
8
‡
80
4
40
2
15000
¶
0
0
¶
¶
Tissue factor and PAI-l concentration in BAL fluid
120
1200
¶
dependent right
lower lobe
75000
p = 0.043
‡
4
0
6 hours
5
§
‡
¶
0
Healthy control
VC 15 mL/kg
VC 6 mL/kg
NAVA
Lung wet to dry ratio
¶
¶
¶
¶
ng/mL
Part IX
Lung wet to dry ratio
814
¶
0
D
FIGURE 35-9 Parameters indicative of ventilator-induced lung injury (VILI) in rabbits with induced acute lung injury (ALI) and ventilated with
three strategies: NAVA, volume control with tidal volume (VT) of 6 mL/kg, and volume control with VT of 15 mL/kg. (A) There were no differences in partial pressure of arterial oxygen to fractional inspired oxygen concentration ratio (PaO2/Fi O2) among groups before and 30 minutes after
induction of ALI. The increase in PaO2/Fi O2 shortly after switching to the assigned ventilation mode (i.e., after randomization into the treatment
groups) was more pronounced with NAVA than with volume control (VC) 6-mL/kg (p < 0.05 post hoc analysis), although PaO2/Fi O2 was not different between NAVA and VC 6-mL/kg at the end of the protocol. With VC 15-mL/kg, PaO2/Fi O2 remained below 200. (B) The lung wet-to-dry ratio
with NAVA and with VC 6-mL/kg was lower than with VC 15-mL/kg (albeit not significantly for the dependent lung in VC 6-mL/kg animals).
(C) and (D) Interleukin 8 (IL-8), tissue factor, and plasminogen activator inhibitor type 1 (PAI-1) concentration in bronchoalveolar (BAL) fluid
was higher in all study groups compared to healthy controls and was higher with VC 15-mL/kg than with the other two groups (except for PAI-1 in
VC 6-mL/kg). Lung tissue IL-8 concentration was increased in all groups as compared to nonventilated controls and was highest in the nondependent lung regions with VC 15-mL/kg. In the VC 6-mL/kg and NAVA groups, lung tissue IL-8 concentration was lower compared to VC 15-mL/kg
(albeit not significant for the dependent lung region). Groups are shown as mean ± standard deviation (SD) for A and B, or as median (quartiles)
for C and D. Symbols represent group mean; bars indicate standard deviation. e–g, time–group interaction (two-way analysis of variance). Post
hoc pairwise comparison procedure between groups: †p <0.05 NAVA versus VC 6-mL/kg; ‡p <0.05 NAVA versus VC 15-mL/kg; §p < 0.05 VC
6-mL/kg versus VC 15-mL/kg. (Used, with permission, from Brander L, Sinderby C, Lecomte F, et al. Neurally adjusted ventilatory assist decreases
ventilator-induced lung injury and non-pulmonary organ dysfunction in rabbits with acute lung injury. Intensive Care Med. 2009;35:1979–1989.)
results indicate that the use of NAVA, which allowed the animals to choose their own respiratory pattern, was at least as
effective in preventing various manifestations of ventilatorinduced lung injury as conventional, volume-controlled ventilation using a tidal volume of 6 mL/kg.
In a human study employing randomized design,
Xirouchaki et al69 ventilated 108 critically ill patients, most of
whom had acute lung injury or acute respiratory distress syndrome, with PAV+ (PAV with automatic estimation of elastance and resistance of the respiratory system; see Chapter
12) Even with high assistance, tidal volume and end-inspiratory plateau pressure were comparable to these observed
during protective controlled mechanical ventilation.
Examination of individual end-inspiratory plateau pressures during PAV+ showed that out of a total of 744 measurements only on nine occasions (1.2%) and in five patients
(4.6%) were plateau pressures above 30 cm H2O (Fig. 35-10).
Ninety-four percent of the end-inspiratory plateau pressures
were below 26 cm H2O, a value associated with lung protection.70 Similar to the findings of Brander et al, these results
can be explained by the operation of reflex feedback (vagally
controlled reflexes).6,63,64
Is it possible to use this reflex feedback into a clinical scenario? Recent studies suggest that in patients with
acute respiratory distress syndrome titration of tidal volume based on individual lung mechanics may be a better
Chapter 35
Effects of Mechanical Ventilation on Control of Breathing
815
40
35
PPLATpav (cm H2O)
30
25
20
15
10
5
–12
0
12
24
36
48
Time (hours)
FIGURE 35-10 Individual values of quasi-static airway pressure obtained by 300 msec pause maneuver at the end of selected inspirations (PPLATpav) as
a function of time in 108 critically ill patients randomized (zero time) to proportional assist ventilation with load-adjustable gain factors (PAV+). PAV+
was continued for 48 hours unless the patients met predefined criteria, either for switching to controlled modes or for breathing without ventilator
assistance. Closed black circles connected by solid thick line represent mean values. Each patient is denoted by a single color. For comparison the mean
± standard deviation (SD) values of static end-inspiratory airway pressure, obtained within 8 hours before randomization during controlled mechanical ventilation (CMV), is shown (closed black square). Notice that in the majority of the patients PPLATpav was below 26 cm H2O. (Used, with permission,
from Kondili et al. Patient–ventilator interaction. Br J Anaesth. 2003;91:106–119.)
strategy than using a fixed tidal volume (i.e., 6 mL/kg).65,66,70–72
Obtaining lung mechanics, however, necessitates the use
of cumbersome techniques not easily available at bedside.
Theoretically, tidal volume selected by the patient should
be based on individual lung mechanics, which serve as a
guide for setting the ventilator.73,74 Although studies support
this hypothesis,68,69 caution should be exercised in patients
with strong signals of nonrespiratory origin (acidosis, brain
dysfunction) that drive ventilation. Notwithstanding the
limitations and feasibility of this approach, this hypothesis
deserves further studies.
Neuromechanical Inhibition
Mechanical ventilation at relatively high tidal volume and
ventilator frequency results in a non–chemically mediated
decrease in respiratory motor output.75–77 This decrease,
referred to as neuromechanical inhibition, is manifested both
in respiratory frequency and in amplitude of respiratory
motor output. Neuromechanical inhibition lasts for several
breaths after termination of mechanical ventilation, thus
constituting a type of control system inertia and resetting of
the spontaneous respiratory rhythm.78 Although the mechanism underlying neuromechanical inhibition is not entirely
clear, the Hering-Breuer reflex is the most plausible explanation. In addition, Sharshar et al79 showed that mechanical ventilation reduces the excitability of cortical motor
areas representing respiratory muscles. It is possible that
mechanoreceptor feedback accounts for the depression of
the motor-evoked potential of the diaphragm via vagal and
other proprioceptive afferents to the respiratory center. The
clinical relevance of neuromechanical inhibition is currently
unknown. Available evidence suggests that its contribution
to respiratory motor output in ventilated critically ill patients
is rather minimal.9,11,55
ENTRAINMENT OF RESPIRATORY
RHYTHM TO VENTILATOR RATE
Entrainment of respiratory rhythm to the ventilator rate
implies a fixed, repetitive, temporal relationship between
the onset of respiratory muscle contraction and the onset
of a mechanical breath.80–82 Human subjects exhibit oneto-one entrainment over a considerable range above and
below the spontaneous breathing frequency.83,84 Cortical
influences (learning or adaptation response) and the
Hering-Breuer reflex are postulated as the predominant
mechanisms of entrainment. Theoretically, one-to-one
entrainment should facilitate patient–ventilator synchrony, but studies of the entrainment response in critically ill patients are lacking.
Behavioral Feedback
The effects of behavioral feedback on control of breathing in ventilated patients are unpredictable, depending
on several factors related to the individual patient and
816
Part IX
Physiologic Effect of Mechanical Ventilation
surroundings. Alteration in ventilator settings, planned
to achieve a particular goal, might be ineffective in awake
patients because of behavioral feedback.85,86 Inappropriate
ventilator settings may cause breathing discomfort in awake
patients. Consequent panic reactions further aggravate the
unpleasant breathing sensation and create a vicious cycle.
Behavioral feedback also may be altered considerably from
time to time secondary to changes in the level of sedation, sleep–awake state, patient status, and environmental
stimuli. The many factors involved in behavioral feedback
complicate its study and the interpretation of its effects on
the system that controls breathing in mechanically ventilated patients.
INTERACTIVE EFFECTS OF PATIENTRELATED FACTORS AND VENTILATOR
ON CONTROL OF BREATHING
Mechanics of Respiratory System
0.8
25
20
15
10
5
0
20
15
10
5
0
–5
Flow (L/s)
Pes (cm H2O)
Paw (cm H2O)
0.8
0.6
0.4
0.2
0
–0.2
–0.4
–0.6
–0.8
Pes (cm H2O)
Flow (L/s)
The mechanical properties of the respiratory system may
influence the pressure delivered by the ventilator independent of patient effort and thus may modify the effects
of mechanical ventilation on the various feedback loops.
Excessive triggering delay and ineffective triggering are
common in patients with obstructive lung disease and
dynamic hyperinflation (Fig. 35-11). In the setting of airflow obstruction, mathematical models predict that PSV
can be accompanied by marked variation in VT and intrinsic
positive end-expiratory pressure even when patient effort
is constant.87 This dynamic instability increases as the time
constant of the respiratory system increases and produces
patient–ventilator asynchrony of variable magnitude and
type. The demonstration of increased arousals during PSV,
but not during volume-cycled ventilation, may be caused in
part by dynamic patient–ventilator asynchrony.21
Ineffective triggering has been observed with all modes
of assisted ventilation. It is particularly common with tachypnea and when the level of assistance is relatively high
and mechanical inflation extends well into neural expiration.11,67,88,89 With PAV and NAVA, the likelihood of ineffective efforts is reduced significantly because mechanical
inflation time is terminated close to the end of neural inspiration, and tidal volume in most cases remains relatively
small.46,47,67,69
The phenomenon of ineffective efforts considerably
influences the interpretation of ventilatory output in relation
to the control of breathing during mechanical ventilation.3,4
In the presence of ineffective efforts, ventilator frequency
does not reflect the patient’s spontaneous respiratory rate
0.6
0.4
0.2
0
–0.2 –0.2
8
6
4
2
0
–0.2 –0.2
–0.4
0.1 0.2 0.3 0.4 0.5 0.6 0.7
0.1 0.2 0.3 0.4 0.5 0.6 0.7
Time (seconds)
Time (seconds)
FIGURE 35-11 Airflow (inspiration up), airway pressure (Paw), and esophageal pressure (Pes) in a patient with obstructive lung disease ventilated
with pressure support. Note the triggering delay with every mechanical breath (see the magnified tracing of flow and Pes) and the ineffective efforts
(arrows). The ventilator rate was 12 breaths/min, whereas the patient’s respiratory frequency was 35 breaths/min. Extrapolation from ventilator rate to
the patient’s system of control of breathing is misleading (Used, with permission, from Springer Science and Business Media: Brander, et al. Intensive
Care Med. 2009;35:1979–1989.)
Chapter 35
(see Fig. 35-11). Moreover, with ineffective efforts, significant alteration in a patient’s respiratory effort occurs secondary to changes in feedback loop.
The characteristics of the Pmus waveform influence the
ventilator-delivered volume in a complex manner, depending on several patient and ventilator factors. Extensive
review of these factors is beyond the scope of this chapter,
but some examples are provided.
The initial rate of increase in Pmus interacts with triggering of the ventilator.11 A low rate of initial increase in Pmus
occurs with a concave upward shape of Pmus or a low respiratory drive (such as with low Pa CO2, sedation, sleep, or a high
level of assistance); this increases the time delay between the
onset of patient inspiratory effort and ventilator triggering
and promotes asynchrony. In the presence of dynamic hyperinflation, a prolonged triggering time, particularly when associated with a relatively short neural inspiratory time and low
peak Pmus, may result in ineffective efforts. Alternatively, an
increase in the intensity of inspiratory effort, such as occurs
with an increase in metabolic rate, high Pa CO2, or decrease
in the level of sedation or assistance, is manifested both in
the rate of rise and in the peak of Pmus. The change may
cause a decrease in the time delay, thus promoting patient–
ventilator synchrony.11 If, however, patient inspiratory effort
is vigorous and longer than mechanical inflation time, the
ventilator may be triggered more than once during the same
inspiratory effort (Fig. 35-12).3,90 It follows that changes in
the characteristics of the Pmus waveform may influence the
ventilator rate and ventilatory output despite no change in a
patient’s breathing frequency. Alterations in ventilatory output may secondarily modify patient effort through changes
in feedback loops (see Fig. 35-1).
THE FUTURE
Over the past two decades, many studies have been performed in animals and human subjects with an aim of
improving a patient’s ability to control the ventilator.
Various ventilator modes target either an improvement in
the response of the ventilator to patient effort or tight coupling between the ventilator-delivered pressure and patient
instantaneous ventilatory demands. Studies of these modes
have yielded promising results. New methods of triggering
have been shown to improve the response of the ventilator
to patient effort.45,91–93 Algorithms that automatically adjust
the criterion for cycling off have been designed with a goal
of reducing expiratory asynchrony.94 Estimates of the inspiratory muscle pressure waveform may also be used to terminate pressure delivery, and these, theoretically, should
improve patient–ventilator synchrony.93 Mechanical92 and
electrical46,95 activity of the diaphragm has been used to
1.5
Flow (L/s)
1.0
0.5
0.0
–0.5
–1.0
Pressure (cm H2O)
Characteristics of the
Muscle Pressure Waveform
817
Effects of Mechanical Ventilation on Control of Breathing
45
40
35
30
25
20
15
10
5
0
–5
–10
Paw
Pes
0
2
4
6
8
10
Time (s)
FIGURE 35-12 Flow, airway pressure (Paw), and esophageal pressure
(Pes) in a patient recovering from acute lung injury and ventilated
on assist volume control at constant inspiratory flow. In the second
breath, tidal volume (volume was not shown) was decreased at constant inspiratory flow. As a result, there was premature termination of
mechanical inspiration. Because the inspiratory muscles continued to
contract, they developed sufficient pressure to overcome elastic recoil
at end inspiration. As a result, Paw decreased below the triggering
threshold, and the ventilator delivered a new mechanical breath. The
ventilator was triggered three times by the two inspiratory efforts.
Note the high Paw of the third mechanical breath secondary to high
lung volume (the volume of the third breath was added to that of the
second). Total breath duration of the second respiratory effort was
considerably longer than that of the first effort owing to activation
of Hering-Breuer reflex by the high volume. (Used, with permission, from Springer Science and Business Media: Xirouchaki, et al.
Intensive Care Med. 2008;34:2026–2034.)
control the level and duration of inspiratory assistance.
With PAV, methods of noninvasive automatic estimation of
elastance and resistance of the respiratory system are now
available (PAV+),96,97 which enable controller gain to be
maintained constant in the face of changes in the mechanical load of respiratory system98 and result in fewer intervention in terms of ventilator settings compared to other
modes.99 Algorithms that use a signal generated from flow,
volume, and airway pressure may be used to provide breathby-breath quantitative information of inspiratory muscle
pressure,100 and this approach also may be used in the future
to facilitate patient–ventilator synchrony. By achieving tight
coupling between neural output and ventilator-delivered
pressure, the ventilator is able to serve as a respiratory muscle with high capabilities and operate in harmony with the
system that controls breathing. Nowadays, it seems feasible
to shift from the physician who dictates the pattern of ventilation to the patient who chooses to breathe with a pattern that incorporates all the aspects of control of breathing.
Because the control of ventilation is much more complex
818
Part IX
Physiologic Effect of Mechanical Ventilation
than simply regulating blood gases, it is likely that the
patient can do a better job than physicians can.
Negative-feedback methods, such as adaptive pressuresupport servoventilation, have been designed recently with
a goal of reducing periodic breathing through appropriate
changes in the level of assistance and maintaining a target
minute ventilation in the face of waxing and waning respiratory efforts.82,101 Incorporation of this approach in assisted
modes may decrease the propensity of high-risk individuals to develop periodic breathing. It is not known whether
this mode could decrease morbidity in critically ill patients,
although it should enhance sleep efficiency.22,23
CONCLUSION
Incorporating an auxiliary pressure into the system that controls breathing changes the volume–time profile of a breath.
It also alters, via chemical, neuromechanical, and behavioral
feedback, the pressure developed by the respiratory muscles.
The latter, depending on ventilator and patient factors, may
or may not modify the auxiliary pressure. The response
of patient effort to a ventilator-delivered breath and the
response of a ventilator to patient effort are the two essential components of control of breathing during mechanical
ventilation. The physician dealing with a ventilated patient
should be aware that both the basic features of control of
breathing and its expression can be altered considerably by
the process of mechanical ventilation.
REFERENCES
1. Tobin MJ. Advances in mechanical ventilation. N Engl J Med.
2001;344:1986–1996.
2. Tobin MJ, Jubran A, Laghi F. Patient-ventilator interaction. Am J
Respir Crit Care Med. 2001;163:1059–1063.
3. Kondili E, Prinianakis G, Georgopoulos D. Patient-ventilator interaction. Br J Anaesth. 2003;91:106–119.
4. Georgopoulos D, Roussos C. Control of breathing in mechanically
ventilated patients. Eur Respir J. 1996;9:2151–2160.
5. Corne S, Bshouty Z. Basic principles of control of breathing. Respir
Care Clin N Am. 2005;11:147–172.
6. Younes M, Remmers J. Control of tidal volume and respiratory frequency. In: Hornbein TF, ed. Regulation of Breathing. New York, NY:
Marcel Dekker; 1981:621–671.
7. Georgopoulos D, Mitrouska I, Webster K, et al. Effects of inspiratory
muscle unloading on the response of respiratory motor output to CO2.
Am J Respir Crit Care Med. 1997;155:2000–2009.
8. Meza S, Giannouli E, Younes M. Control of breathing during sleep
assessed by proportional assist ventilation. J Appl Physiol. 1998;84:
3–12.
9. Xirouhaki N, Kondili E, Mitrouska I, et al. Response of respiratory
motor output to varying pressure in mechanically ventilated patients.
Eur Respir J. 1999;14:508–516.
10. Skatrud JB, Berssenbrugge AD. Effect of sleep state and chemical stimuli on breathing. Prog Clin Biol Res. 1983;136:87–95.
11. Leung P, Jubran A, Tobin MJ. Comparison of assisted ventilator modes
on triggering, patient effort, and dyspnea. Am J Respir Crit Care Med.
1997;155:1940–1948.
12. Cunningham DJC RP, Robbins PA, Wolff CB. Integration of
Respiratory Responses to Changes in Alveolar Partial Pressures of CO2
and O2 and in the Arterial pH. Bethesda, MD: American Physiological
Society; 1986.
13. Georgopoulos D, Mitrouska I, Bshouty Z, et al. Respiratory response
to CO2 during pressure-support ventilation in conscious normal
humans. Am J Respir Crit Care Med. 1997;156:146–154.
14. Puddy A, Patrick W, Webster K, Younes M. Respiratory control during volume-cycled ventilation in normal humans. J Appl Physiol.
1996;80:1749–1758.
15. Patrick W, Webster K, Puddy A, et al. Respiratory response to
CO2 in the hypocapnic range in awake humans. J Appl Physiol.
1995;79:2058–2068.
16. Mitrouska J, Xirouchaki N, Patakas D, et al. Effects of chemical
feedback on respiratory motor and ventilatory output during different modes of assisted mechanical ventilation. Eur Respir J. 1999;13:
873–882.
17. Dempsey JA, Skatrud JB. A sleep-induced apneic threshold and its
consequences. Am Rev Respir Dis. 1986;133:1163–1170.
18. Dempsey JA, Smith CA, Przybylowski T, et al. The ventilatory responsiveness to CO(2) below eupnoea as a determinant of ventilatory stability in sleep. J Physiol. 2004;560:1–11.
19. Meza S, Mendez M, Ostrowski M, Younes M. Susceptibility to periodic
breathing with assisted ventilation during sleep in normal subjects.
J Appl Physiol. 1998;85:1929–1940.
20. Corne S, Webster K, Younes M. Hypoxic respiratory response
during acute stable hypocapnia. Am J Respir Crit Care Med.
2003;167:1193–1199.
21. Parthasarathy S, Tobin MJ. Effect of ventilator mode on sleep quality in
critically ill patients. Am J Respir Crit Care Med. 2002;166:1423–1429.
22. Parthasarathy S, Tobin MJ. Sleep in the intensive care unit. Intensive
Care Med. 2004;30:197–206.
23. Alexopoulou C, Kondili E, Vakouti E, et al. Sleep during proportionalassist ventilation with load-adjustable gain factors in critically ill
patients. Intensive Care Med. 2007;33:1139–1147.
24. Sin DD, Logan AG, Fitzgerald FS, et al. Effects of continuous positive airway pressure on cardiovascular outcomes in heart failure
patients with and without Cheyne-Stokes respiration. Circulation.
2000;102:61–66.
25. Leung RS, Bradley TD. Sleep apnea and cardiovascular disease. Am J
Respir Crit Care Med. 2001;164:2147–2165.
26. McGuire BE, Basten CJ, Ryan CJ, Gallagher J. Intensive care unit syndrome: a dangerous misnomer. Arch Intern Med. 2000;160:906–909.
27. Helton MC, Gordon SH, Nunnery SL. The correlation between
sleep deprivation and the intensive care unit syndrome. Heart Lung.
1980;9:464–468.
28. Irwin M, McClintick J, Costlow C, et al. Partial night sleep deprivation reduces natural killer and cellular immune responses in humans.
FASEB J. 1996;10:643–653.
29. Irwin M, Rinetti G, Redwine L, et al. Nocturnal proinflammatory
cytokine-associated sleep disturbances in abstinent African American
alcoholics. Brain Behav Immun. 2004;18:349–360.
30. Redwine L, Hauger RL, Gillin JC, Irwin M. Effects of sleep and sleep
deprivation on interleukin-6, growth hormone, cortisol, and melatonin levels in humans. J Clin Endocrinol Metab. 2000;85:3597–3603.
31. Scrimshaw NS, Habicht JP, Pellet P, et al. Effects of sleep deprivation
and reversal of diurnal activity on protein metabolism of young men.
Am J Clin Nutr. 1966;19:313–319.
32. Khoo MC, Kronauer RE, Strohl KP, Slutsky AS. Factors inducing periodic breathing in humans: a general model. J Appl Physiol.
1982;53:644–659.
33. Younes M, Ostrowski M, Thompson W, et al. Chemical control stability in patients with obstructive sleep apnea. Am J Respir Crit Care Med.
2001;163:1181–1190.
34. Grace MP, Greenbaum DM. Cardiac performance in response to PEEP
in patients with cardiac dysfunction. Crit Care Med. 1982;10:358–360.
35. Lenique F, Habis M, Lofaso F, et al. Ventilatory and hemodynamic
effects of continuous positive airway pressure in left heart failure. Am
J Respir Crit Care Med. 1997;155:500–505.
36. Pinsky MR. Instantaneous venous return curves in an intact canine
preparation. J Appl Physiol. 1984;56:765–771.
37. Pinsky MR. The effects of mechanical ventilation on the cardiovascular system. Crit Care Clin. 1990;6:663–678.
38. Mansfield D, Naughton MT. Effects of continuous positive airway
pressure on lung function in patients with chronic obstructive pulmonary disease and sleep disordered breathing. Respirology. 1999;4:
365–370.
Chapter 35
39. Javaheri S. Effects of continuous positive airway pressure on sleep
apnea and ventricular irritability in patients with heart failure.
Circulation. 2000;101:392–397.
40. Kohnlein T, Welte T, Tan LB, Elliott MW. Assisted ventilation for
heart failure patients with Cheyne-Stokes respiration. Eur Respir J.
2002;20:934–941.
41. Klimathianaki M, Kondili E, Alexopoulou C, et al. Effect of propofol
on breathing stability in adult ICU patients with brain damage. Respir
Physiol Neurobiol. 2010;171:232–238.
42. Nakayama H, Smith CA, Rodman JR, et al. Effect of ventilatory drive
on carbon dioxide sensitivity below eupnea during sleep. Am J Respir
Crit Care Med. 2002;165:1251–1260.
43. ATS/ERS Statement on respiratory muscle testing. Am J Respir Crit
Care Med. 2002;166:518–624.
44. Otis A. Quantitative relationships in steady state gas exchange. In:
Fenn WO, Rahn H, eds. Handbook of Physiology: Respiration. Vol. I.
Washington, DC: American Physiological Society; 1964:681–698.
45. Sinderby C, Navalesi P, Beck J, et al. Neural control of mechanical ventilation in respiratory failure. Nat Med. 1999;5:1433–1436.
46. Colombo D, Cammarota G, Bergamaschi V, et al. Physiologic response
to varying levels of pressure support and neurally adjusted ventilatory
assist in patients with acute respiratory failure. Intensive Care Med.
2008;34:2010–2018.
47. Terzi N, Pelieu I, Guittet L, et al. Neurally adjusted ventilatory assist
in patients recovering spontaneous breathing after acute respiratory distress syndrome: physiological evaluation. Crit Care Med.
2010;38:1830–1837.
48. Bosma K, Ferreyra G, Ambrogio C, et al. Patient-ventilator interaction and sleep in mechanically ventilated patients: pressure support versus proportional assist ventilation. Crit Care Med. 2007;35:
1048–1054.
49. Wellman A, Jordan AS, Malhotra A, et al. Ventilatory control and airway anatomy in obstructive sleep apnea. Am J Respir Crit Care Med.
2004;170:1225–1232.
50. Wellman A, Malhotra A, Fogel RB, et al. Respiratory system loop gain
in normal men and women measured with proportional-assist ventilation. J Appl Physiol. 2003;94:205–212.
51. Georgopoulus D, Giannouli E, Tsara V, et al. Respiratory short-term
poststimulus potentiation (after-discharge) in patients with obstructive sleep apnea. Am Rev Respir Dis. 1992;146:1250–1255.
52. Ranieri VM, Giuliani R, Mascia L, et al. Patient-ventilator interaction
during acute hypercapnia: pressure-support vs. proportional-assist
ventilation. J Appl Physiol. 1996;81:426–436.
53. Younes M, Riddle W. Relation between respiratory neural output and
tidal volume. J Appl Physiol. 1984;56:1110–1119.
54. Fauroux B, Hart N, Luo YM, et al. Measurement of diaphragm loading during pressure support ventilation. Intensive Care Med. 2003;
29:1960–1966.
55. Kondili E, Prinianakis G, Anastasaki M, Georgopoulos D. Acute
effects of ventilator settings on respiratory motor output in patients
with acute lung injury. Intensive Care Med. 2001;27:1147–1157.
56. Georgopoulos D, Mitrouska I, Bshouty Z, et al. Effects of non-REM
sleep on the response of respiratory output to varying inspiratory flow.
Am J Respir Crit Care Med. 1996;153:1624–1630.
57. Georgopoulos D, Mitrouska I, Bshouty Z, et al. Effects of breathing
route, temperature and volume of inspired gas, and airway anesthesia
on the response of respiratory output to varying inspiratory flow. Am J
Respir Crit Care Med. 1996;153:168–175.
58. Fernandez R, Mendez M, Younes M. Effect of ventilator flow rate on
respiratory timing in normal humans. Am J Respir Crit Care Med.
1999;159:710–719.
59. Corne S, Webster K, Younes M. Effects of inspiratory flow on
diaphragmatic motor output in normal subjects. J Appl Physiol.
2000;89:481–492.
60. Tobert DG, Simon PM, Stroetz RW, Hubmayr RD. The determinants
of respiratory rate during mechanical ventilation. Am J Respir Crit
Care Med. 1997;155:485–492.
61. Younes M, Kun J, Webster K, Roberts D. Response of ventilatordependent patients to delayed opening of exhalation valve. Am J Respir
Crit Care Med. 2002;166:21–30.
62. Corne S, Gillespie D, Roberts D, Younes M. Effect of inspiratory flow
rate on respiratory rate in intubated ventilated patients. Am J Respir
Crit Care Med. 1997;156:304–308.
Effects of Mechanical Ventilation on Control of Breathing
819
63. Bartlett D Jr, St John WM. Influence of lung volume on phrenic, hypoglossal and mylohyoid nerve activities. Respir Physiol. 1988;73:97–109.
64. Kuna ST. Inhibition of inspiratory upper airway motoneuron activity
by phasic volume feedback. J Appl Physiol. 1986;60:1373–1379.
65. Caironi P, Cressoni M, Chiumello D, et al. Lung opening and closing
during ventilation of acute respiratory distress syndrome. Am J Respir
Crit Care Med. 2010;181:578–586.
66. Chiumello D, Carlesso E, Cadringher P, et al. Lung stress and strain
during mechanical ventilation for acute respiratory distress syndrome.
Am J Respir Crit Care Med. 2008;178:346–355.
67. Giannouli E, Webster K, Roberts D, Younes M. Response of ventilatordependent patients to different levels of pressure support and proportional assist. Am J Respir Crit Care Med. 1999;159:1716–1725.
68. Brander L, Sinderby C, Lecomte F, et al. Neurally adjusted ventilatory
assist decreases ventilator-induced lung injury and non-pulmonary
organ dysfunction in rabbits with acute lung injury. Intensive Care
Med. 2009;35:1979–1989.
69. Xirouchaki N, Kondili E, Vaporidi K, et al. Proportional assist ventilation with load-adjustable gain factors in critically ill patients: comparison with pressure support. Intensive Care Med. 2008;34:2026–2034.
70. Terragni PP, Rosboch G, Tealdi A, et al. Tidal hyperinflation during
low tidal volume ventilation in acute respiratory distress syndrome.
Am J Respir Crit Care Med. 2007;175:160–166.
71. Talmor D, Sarge T, Malhotra A, et al. Mechanical ventilation
guided by esophageal pressure in acute lung injury. N Engl J Med.
2008;359:2095–2104.
72. Grasso S, Stripoli T, De Michele M, et al. ARDSnet ventilatory protocol and alveolar hyperinflation: role of positive end-expiratory pressure. Am J Respir Crit Care Med. 2007;176:761–767.
73. Brochard LJ. Tidal volume during acute lung injury: let the patient
choose? Intensive Care Med. 2009;35:1830–1832.
74. Leiter JC, Manning HL. The Hering-Breuer reflex, feedback control,
and mechanical ventilation: the promise of neurally adjusted ventilatory assist. Crit Care Med. 2010;38:1915–1916.
75. Wilson CR, Satoh M, Skatrud JB, Dempsey JA. Non-chemical inhibition of respiratory motor output during mechanical ventilation in
sleeping humans. J Physiol. 1999;518 (Pt 2):605–618.
76. Leevers AM, Simon PM, Dempsey JA. Apnea after normocapnic mechanical ventilation during NREM sleep. J Appl Physiol.
1994;77:2079–2085.
77. Manchanda S, Leevers AM, Wilson CR, et al. Frequency and volume
thresholds for inhibition of inspiratory motor output during mechanical ventilation. Respir Physiol. 1996;105:1–16.
78. Rice AJ, Nakayama HC, Haverkamp HC, et al. Controlled versus
assisted mechanical ventilation effects on respiratory motor output in
sleeping humans. Am J Respir Crit Care Med. 2003;168:92–101.
79. Sharshar T, Ross ET, Hopkinson NS, et al. Depression of diaphragm
motor cortex excitability during mechanical ventilation. J Appl Physiol.
2004;97:3–10.
80. Petrillo GA, Glass L. A theory for phase locking of respiration in cats
to a mechanical ventilator. Am J Physiol. 1984;246:R311–R320.
81. Muzzin S, Trippenbach T, Baconnier P, Benchetrit G. Entrainment of
the respiratory rhythm by periodic lung inflation during vagal cooling.
Respir Physiol. 1989;75:157–172.
82. Muzzin S, Baconnier P, Benchetrit G. Entrainment of respiratory
rhythm by periodic lung inflation: effect of airflow rate and duration.
Am J Physiol. 1992;263:R292–R300.
83. Simon PM, Habel AM, Daubenspeck JA, Leiter JC. Vagal feedback in
the entrainment of respiration to mechanical ventilation in sleeping
humans. J Appl Physiol. 2000;89:760–769.
84. Simon PM, Zurob AS, Wies WM, et al. Entrainment of respiration
in humans by periodic lung inflations. Effect of state and CO2. Am J
Respir Crit Care Med. 1999;160:950–960.
85. Manning HL, Molinary EJ, Leiter JC. Effect of inspiratory flow rate on
respiratory sensation and pattern of breathing. Am J Respir Crit Care
Med. 1995;151:751–757.
86. Jubran A, Van de Graaff WB, Tobin MJ. Variability of patient-ventilator interaction with pressure support ventilation in patients with
chronic obstructive pulmonary disease. Am J Respir Crit Care Med.
1995;152:129–136.
87. Hotchkiss JR Jr, Adams AB, Stone MK, et al. Oscillations and noise:
inherent instability of pressure support ventilation? Am J Respir Crit
Care Med. 2002;165:47–53.
820
Part IX
Physiologic Effect of Mechanical Ventilation
88. Thille AW, Cabello B, Galia F, et al. Reduction of patient-ventilator
asynchrony by reducing tidal volume during pressure-support ventilation. Intensive Care Med. 2008;34:1477–1486.
89. Thille AW, Rodriguez P, Cabello B, et al. Patient-ventilator asynchrony during assisted mechanical ventilation. Intensive Care Med.
2006;32:1515–1522.
90. Georgopoulos D, Prinianakis G, Kondili E. Bedside waveforms interpretation as a tool to identify patient-ventilator asynchronies. Intensive
Care Med. 2006;32:34–47.
91. Prinianakis G, Kondili E, Georgopoulos D. Effects of the flow
waveform method of triggering and cycling on patient-ventilator
interaction during pressure support. Intensive Care Med. 2003;29:
1950–1959.
92. Sharshar T, Desmarais G, Louis B, et al. Transdiaphragmatic pressure
control of airway pressure support in healthy subjects. Am J Respir Crit
Care Med. 2003;168:760–769.
93. Younes M, Brochard L, Grasso S, et al. A method for monitoring and
improving patient: ventilator interaction. Intensive Care Med. 2007;
33:1337–1346.
94. Du HL, Amato MB, Yamada Y. Automation of expiratory trigger
sensitivity in pressure support ventilation. Respir Care Clin N Am.
2001;7:503–517, x.
95. Spahija J, Beck J, de Marchie M, et al. Closed-loop control of respiratory drive using pressure-support ventilation: target drive ventilation.
Am J Respir Crit Care Med. 2005;171:1009–1014.
96. Younes M, Kun J, Masiowski B, et al. A method for noninvasive determination of inspiratory resistance during proportional assist ventilation. Am J Respir Crit Care Med. 2001;163:829–839.
97. Younes M, Webster K, Kun J, et al. A method for measuring passive
elastance during proportional assist ventilation. Am J Respir Crit Care
Med. 2001;164:50–60.
98. Kondili E, Prinianakis G, Alexopoulou C, et al. Respiratory load
compensation during mechanical ventilation-proportional assist
ventilation with load-adjustable gain factors versus pressure support.
Intensive Care Med. 2006;32:692–699.
99. Xirouchaki N, Kondili E, Klimathianaki M, Georgopoulos D. Is proportional-assist ventilation with load-adjustable gain factors a userfriendly mode? Intensive Care Med. 2009;35:1599–1603.
100. Kondili E, Alexopoulou C, Xirouchaki N, et al. Estimation of inspiratory muscle pressure in critically ill patients. Intensive Care Med.
2010;36:648–655.
101. Pepperell JC, Maskell NA, Jones DR, et al. A randomized controlled
trial of adaptive ventilation for Cheyne-Stokes breathing in heart failure. Am J Respir Crit Care Med. 2003;168:1109–1114.
EFFECT OF MECHANICAL
VENTILATION ON HEART–LUNG
INTERACTIONS
36
Hernando Gomez
Michael R. Pinsky
CLINICAL RELEVANCE
PHYSIOLOGY OF HEART–LUNG INTERACTIONS
Effect of Lung Volume
Effect of Intrathoracic Pressure
SPONTANEOUS BREATHING VERSUS MECHANICAL
POSITIVE-PRESSURE VENTILATION
DETECTION AND MONITORING
Weaning Failure
Using Ventilation to Define Cardiovascular Performance
CLINICAL SCENARIOS
Initiating Mechanical Ventilation
Comparing Different Ventilator Modes
Upper Airway Obstruction
Chronic Obstructive Pulmonary Disease
Auto–Positive End-Expiratory Pressure
The heart and lungs are intimately coupled by their anatomical proximity within the thorax and, more importantly, by
their responsibility to deliver the O2 requirements of individual cells and organs while excreting the CO2 by-product
of metabolism. During critical illness, if these two organ systems fail, either alone or in combination, the end result is
an inadequate O2 delivery to the body with inevitable tissue
ischemia, progressive organ dysfunction, and if untreated,
death. Thus, restoration and maintenance of normalized cardiopulmonary function is an essential and primary goal in
the management of critically ill patients. Heart failure can
impair gas exchange by inducing pulmonary edema and limiting blood flow to the respiratory muscles. Ventilation can
alter cardiovascular function by altering lung volume, and
intrathoracic pressure (ITP), and by increasing metabolic
demands. These processes are discussed from the perspective of the impact that ventilation has on the cardiovascular
system.
Acute Respiratory Distress Syndrome and Acute Lung Injury
Congestive Heart Failure
Intraoperative State
STEPS TO LIMIT OR OVERCOME DETRIMENTAL
HEART–LUNG INTERACTIONS
Minimize Work of Breathing
Minimize Negative Swings in Intrathoracic Pressure
Prevent Hyperinflation
Fluid Resuscitation during Initiation of Positive-Pressure
Ventilation
Prevent Volume Overload during Weaning
Augment Cardiac Contractility
IMPORTANT UNKNOWNS
THE FUTURE
SUMMARY AND CONCLUSIONS
CLINICAL RELEVANCE
The ventilatory apparatus and the cardiovascular system have
profound effects on each other.1,2 Acute hypoxia impairs cardiac contractility and vascular smooth muscle tone, promoting cardiovascular collapse. Hypercarbia causes vasodilation
and increases pulmonary vascular resistance. Hyperinflation
increases pulmonary vascular resistance, which impedes
right-ventricular (RV) ejection and also compresses the heart
inside the cardiac fossa in a fashion analogous to tamponade.
Lung collapse also increases pulmonary vascular resistance,
impeding RV ejection.3 Acute RV failure, or cor pulmonale,
is not only difficult to treat, but it can induce immediate
cardiovascular collapse and death.
Ventilator technologies and numerous vasoactive drugs
have been developed as means to improve oxygenation
of arterial blood. These advances are the subjects of other
chapters in this volume. The complex interactions, however,
821
822
Part IX
Physiologic Effect of Mechanical Ventilation
between the heart, circulation, and lungs often leads to a paradoxical worsening of one organ system function while the
function of the other is either maintained or even improved
by the use of these technologies and drugs. To minimize
these deleterious events, and in the hope of more efficiently
and effectively treating critical ill patients with cardiorespiratory failure, a better knowledge and understanding of the
integrated behavior of the cardiopulmonary system, during both health and critical illness is essential. Based on this
perspective, the health care provider can more appropriately
manage this complex and challenging group of patients.
Respiratory function alters cardiovascular function and
cardiovascular function alters respiratory function. A useful
way to consider the cardiovascular effects of ventilation is
to group them by their impact on the determinants of cardiac performance. The determinants of cardiac function
can be grouped into four interrelated processes: heart rate,
preload, contractility, and afterload. Phasic changes in lung
volume and ITP can simultaneously change all four of these
hemodynamic determinants for both ventricles. Our current
understanding of cardiovascular function also emphasizes
both the independence and interdependence of RV and leftventricular (LV) performance on each other and to external
stresses. Complicating these matters further, the direction of
interdependence, from right to left or left to right, can be
similar or opposite in direction, depending on the baseline
cardiovascular state. It is clear, therefore, that a comprehensive understanding of the specific cardiopulmonary interactions and their relative importance in defining a specific
cardiovascular state is a nearly impossible goal to achieve
in most patients. By understanding the components of this
process, however, one can come to a better realization of its
determinants, and, to a greater or lesser degree for any individual patient, predict the limits of these interactions and
how the patient may respond to stresses imposed by either
adding or removing artificial ventilatory support.
PHYSIOLOGY OF HEART–LUNG
INTERACTIONS
Both spontaneous and positive-pressure ventilation increase
lung volume above an end-expiratory baseline. Many of the
hemodynamic effects of all forms of ventilation are similar
despite differences in the mode of ventilation. ITP, however,
decreases during spontaneous inspiration and increases during positive-pressure ventilation. Thus, the primary reasons
for different hemodynamic responses seen during spontaneous and positive-pressure breathing are related to the changes
in ITP and the energy necessary to produce those changes.
Effect of Lung Volume
Changing lung volume phasically alters autonomic tone and
pulmonary vascular resistance. At very high lung volumes,
the expanding lungs compress the heart in the cardiac fossa,
limiting absolute cardiac volumes analogous to cardiac tamponade, except that with hyperinflation both pericardial
pressure and ITP increase by a similar amount.
AUTONOMIC TONE
Although neurohumoral processes define a few immediate effects of ventilation on the heart, these neurohumoral
processes probably play a primary role in all the long-term
effects of ventilation on the cardiovascular system. Most
of the immediate effects of ventilation of the heart are secondary to changes in autonomic tone. The lungs are richly
enervated with somatic and autonomic fibers that originate,
traverse through, and end in the thorax. These networks
mediate multiple homeostatic processes through the autonomic nervous system altering instantaneous cardiovascular
function. The most commonly known of these are the vagally
mediated heart rate changes during ventilation.4,5 Inflation
of the lung to normal tidal volumes (<10 mL/kg) induces
vagal-tone withdrawal, accelerating heart rate. This phenomenon is known as respiratory sinus arrhythmia6 and can
be used to document normal autonomic control,7 especially
in patients with diabetes who are at risk for peripheral neuropathy.8 Inflation to larger tidal volumes (>15 mL/kg), however, decreases heart rate by a combination of both increased
vagal tone9 and sympathetic withdrawal. Sympathetic withdrawal also creates arterial vasodilation.4,10–14 This inflation–
vasodilation response can reduce LV contractility in healthy
volunteers15 and in ventilator-dependent patients with the
initiation of high-frequency ventilation4 or hyperinflation.12
This inflation–vasodilation response is presumed to be the
cause of the initial hypotension seen when infants are placed
on mechanical ventilation. It appears to be mediated at least
partially by afferent vagal fibers, because it is abolished by
selective vagotomy. Hexamethonium, guanethidine, and bretylium, however, also block this reflex.16,17 These data suggest that lung inflation mediates its reflex cardiovascular
effects by modulating central autonomic tone. Interestingly,
the almost total lack of measurable hemodynamic effects
of unilateral hyperinflation in subjects with normal lungs
receiving split-lung ventilation18 suggests that these autonomic cardiovascular effects require a general increase in
lung volume to be realized. This is not a minor point because
selective hyperinflation within lung units commonly occurs
in patients with acute lung injury (ALI) and chronic obstructive pulmonary disease (COPD). If localized hyperinflation
were able to induce cardiovascular impairment, these subjects would be profoundly compromised.
Humoral factors, including compounds blocked by
cyclooxygenase inhibition,19 released from pulmonary
endothelial cells during lung inflation may also induce
this depressor response20–22 within a short (15 seconds)
time frame. These interactions, however, do not appear
to grossly alter cardiovascular status.23 Ventilation also
alters the more chronic control of intravascular fluid
balance via hormonal release. The right atrium functions as the body’s effective circulating blood-volume
Chapter 36 Effect of Mechanical Ventilation on Heart–Lung Interactions
sensor. Circulating levels of a family of natriuretic peptides increase in heart failure states secondary to rightatrial stretch.24 These hormones promote sodium and
water diuresis. The levels of these hormones vary directly
with the degree of heart failure. Both positive-pressure
ventilation and sustained hyperinflation decrease rightatrial stretch mimicking hypovolemia. During positivepressure ventilation, plasma norepinephrine and renin
increase,25,26 whereas atrial natriuretic peptide decreases.27
This humoral response is the primary reason why ventilator-dependent patients gain weight early in the course
of respiratory failure, because protein catabolism is also
usually seen. Interestingly, when patients with congestive
heart failure (CHF) are given nasal continuous positive
airway pressure (CPAP), plasma atrial natriuretic peptide
activity decreases in parallel with improvements in blood
flow.28,29 This finding suggests that some of the observed
benefit of CPAP therapy in heart failure is mediated in
part through humoral mechanisms, owing to the mechanical effects of CPAP on cardiac function.
PULMONARY VASCULAR RESISTANCE
Changing lung volume alters pulmonary vascular resistance.3
Marked increases in pulmonary vascular resistance, as may
occur with hyperinflation, can induce acute cor pulmonale
and cardiovascular collapse. The reasons for these changes
are multifactorial. They can reflect conflicting cardiovascular processes and almost always reflect both humoral and
mechanical interactions.
Lung volume can only increase if its distending pressure
increases. Lung-distending pressure, called the transpulmonary pressure, equals the pressure difference between alveolar pressure (Palv) and ITP. If lung volume does not change,
then transpulmonary pressure does not change. Thus,
occluded inspiratory efforts (Mueller maneuver) and expiratory efforts (Valsalva maneuver) cause ITP to vary by an
amount equal to Palv, but do not change pulmonary vascular
resistance. Although obstructive inspiratory efforts, as occur
during obstructive sleep apnea, are usually associated with
increased RV afterload, the increased afterload is caused primarily by either increased vasomotor tone (hypoxic pulmonary vasoconstriction) or backward LV failure.30,31
RV afterload is maximal RV systolic wall stress.32,33 By
law of Laplace, wall stress equals the product of the radius of
curvature of a structure and its transmural pressure. Systolic
RV pressure equals transmural pulmonary artery pressure.
Increases in transmural pulmonary artery pressure increases
RV afterload, impeding RV ejection,34 decreasing RV stroke
volume,35 inducing RV dilation, and passively causing venous
return to decrease.19,21 If such acute increases in transmural
pulmonary artery pressure are not reduced, or if RV contractility is not increased by artificial means, then acute cor
pulmonale rapidly develops.36 If RV dilation and RV pressure overload persist, RV free-wall ischemia and infarction
can develop.37 These concepts are of profound clinical relevance because rapid fluid challenges in the setting of acute
823
cor pulmonale can precipitate profound cardiovascular collapse secondary to excessive RV dilation, RV ischemia, and
compromised LV filling. Ventilation can alter pulmonary
vascular resistance by either altering pulmonary vasomotor
tone, via a process known as hypoxic pulmonary vasoconstriction, or mechanically altering vessel cross-sectional area, by
changing transpulmonary pressure.
Hypoxic Pulmonary Vasoconstriction. Unlike systemic
vessels that dilate under hypoxic conditions, the pulmonary
vasculature constricts. Once alveolar partial pressure of
oxygen decreases below 60 mm Hg, or acidemia develops,
pulmonary vasomotor tone increases.38 Hypoxic pulmonary
vasoconstriction is mediated, in part, by variations in the
synthesis and release of nitric oxide by endothelial nitric
oxide synthase localized on pulmonary vascular endothelial
cells, and in part by changes in intracellular calcium fluxes
in the pulmonary vascular smooth muscle cells. The
pulmonary endothelium normally synthesizes a low basal
amount of nitric oxide, keeping the pulmonary vasculature
actively vasodilated. Loss of nitric oxide allows the smooth
muscle to return to its normal resting vasomotor tone. Nitric
oxide synthesis is dependent on adequate amounts of O2
and is inhibited by both hypoxia and acidosis. Presumably,
hypoxic pulmonary vasoconstriction developed to minimize
ventilation–perfusion mismatches caused by local alveolar
hypoventilation. Generalized alveolar hypoxia, however,
increases global pulmonary vasomotor tone, impeding
RV ejection.32 At low lung volumes, terminal bronchioles
collapse, trapping gas in the terminal alveoli. With continued
blood flow, these alveoli lose their O2 and also may collapse.
Patients with acute hypoxemic respiratory failure have small
lung volumes and are prone to both alveolar hypoxia and
spontaneous alveolar collapse.39,40 This is one of the main
reasons why pulmonary vascular resistance is increased in
patients with acute hypoxemic respiratory failure.
Based on the above considerations, mechanical ventilation may reduce pulmonary vasomotor tone by a variety of
mechanisms. First, hypoxic pulmonary vasoconstriction can
be inhibited if the patient is ventilated with gas enriched with
O2 increasing alveolar partial pressure of oxygen.41–44 Second,
mechanical breaths and positive end-expiratory pressure
(PEEP) can refresh hypoventilated lung units and recruit collapsed alveolar units, causing local increases in alveolar partial pressure of oxygen,3,45–47 especially if small lung volumes
are returned to resting functional residual capacity (FRC)
from an initial smaller lung volume.48 Third, mechanical
ventilation often reverses respiratory acidosis by increasing
alveolar ventilation.44 Fourth, decreasing central sympathetic
output, by sedation or decreased stress of breathing against
high-input impedance during mechanical ventilation, also
reduces vasomotor tone.49,50 Importantly, these effects do not
require endotracheal intubation to occur; they occur with
mere reexpansion of collapsed alveoli.51,52 Thus, PEEP, CPAP,
recruitment maneuvers, and noninvasive ventilation may
all reverse hypoxic pulmonary vasoconstriction and may all
improve cardiovascular function.
824
Part IX
Physiologic Effect of Mechanical Ventilation
Pulmonary vascular resistance
Volume-Dependent Changes in Pulmonary Vascular
Resistance. Changes in lung volume directly alter pulmonary vasomotor tone by compressing the alveolar
vessels.39,46,47 The actual mechanisms by which this occurs
have not been completely resolved, but appear to reflect
vascular compression induced by a differential extraluminal
pressure gradient. The pulmonary circulation lives in two
environments, separated from each other by the pressure
that surrounds them.46 The small pulmonary arterioles,
venules, and alveolar capillaries sense Palv as their
surrounding pressure, and are called alveolar vessels. The
large pulmonary arteries and veins, as well as the heart and
intrathoracic great vessels of the systemic circulation, sense
interstitial pressure or ITP as their surrounding pressure,
and are called extraalveolar vessels. Because the pressure
difference between Palv and ITP is transpulmonary
pressure, increasing lung volume increases this extraluminal
pressure gradient. Increases in lung volume progressively
increase alveolar vessel resistance by increasing this
pressure difference once lung volumes increase much above
FRC (Fig. 36-1).42,53 Similarly, increasing lung volume,
by stretching and distending the alveolar septa, may also
compress alveolar capillaries, although this mechanism is
less well substantiated. Hyperinflation can create significant
pulmonary hypertension and may precipitate acute RV
failure (acute cor pulmonale)54 and RV ischemia.37 Thus,
PEEP may increase pulmonary vascular resistance if it
induces overdistension of the lung above its normal FRC.55
Extraalveolar vessels are also influenced by changes in
transpulmonary pressure. Normally, radial interstitial forces
of the lung, which keep the airways patent, only make the large
Total PVR
Alveolar
compression
Hypoxic
pulmonary
vasoconstriction
vessels more distended as lung volume increases,45,56,57 just
as increasing lung volume increases airway diameter. These
radial forces also act upon the extraalveolar vessels, causing
them to remain dilated, increasing their capacitance.58 This
tethering is reversed with lung deflation, thereby increasing
extraalveolar vascular resistance.42,45 Thus, pulmonary vascular resistance is increased at small lung volumes owing to
the combined effect of hypoxic pulmonary vasoconstriction
and extraalveolar vessel collapse, and at high lung volumes
by alveolar compression.
Right-Ventricular Afterload. The right ventricle, as
opposed to the left ventricle, ejects blood into a low-pressure,
high-compliance system: the pulmonary circulation. The
pulmonary circulation is capable of accommodating high
volumes of blood without generating high pressure, which
is beneficial for the right ventricle. Despite being compliant,
this circuit does pose resistance to the ejecting right ventricle
as quantified by pulmonary artery pressure, which is the
pressure limit the right ventricle has to overcome to open
the pulmonary valve. RV afterload is conceptually similar
to LV afterload and is determined by the wall tension of
the right ventricle. RV afterload is highly dependent on the
distribution of blood flow in the lung, namely, the proportion
of West zones 1 and 2, as compared to zone 3, as originally
described by Permutt et al.59 Zones 1 and 2 exist whenever
the intraluminal pressure of juxtaalveolar capillaries is lower
than the Palv during the respiratory cycle, thus collapsing
vessels and increasing pulmonary vascular resistance. In
contrast, zone 3 occurs when intraluminal capillary pressure
is higher than Palv, decreasing pulmonary resistance.
Importantly, intraluminal pressure of alveolar capillaries
tracks changes in ITP,60 and thus decreases less than Palv
during spontaneous inspiration, and increases less than Palv
during positive-pressure inspiration. Consequently, both
spontaneous and positive-pressure inspiration above FRC
increase the afterload to the right ventricle as opposed to
the LV afterload, which is reduced by increased ITP.
VENTRICULAR INTERDEPENDENCE
Extraalveolar
vessels
Alveolar
vessels
Residual
volume
Functional
residual
capacity
Total
lung
capacity
Lung volume
FIGURE 36-1 Schematic of the relationship between changes in lung
volume and pulmonary vascular resistance (PVR), where the extraalveolar and alveolar vascular components are separated. Pulmonary
vascular resistance is minimal at resting lung volume or functional
residual capacity. As lung volume increases toward total lung capacity or decreases toward residual volume, pulmonary vascular resistance
also increases. The increase in resistance with hyperinflation is caused
by increased alveolar vascular resistance, whereas the increase in resistance with lung collapse is caused by increased extraalveolar vessel tone.
Because right ventricle output is linked to left ventricle output serially, if right ventricle output decreases, left ventricle
output must eventually decrease. The two ventricles, however, are also linked in parallel through their common septum, circumferential fibers, and pericardium, which limits
total cardiac volume. For this reason, the diastolic filling
of the RV has a direct influence on the shape and compliance of the LV, and vice versa. This phenomenon is known
as ventricular diastolic interdependence.61 The most common
manifestation of ventricular interdependence is pulsus paradoxus. Changes in RV end-diastolic volume inversely alter
LV diastolic compliance.62 Because venous return can and
often does vary by as much as 200% between inspiration and
expiration, owing to associated changes in the pressure gradient for venous return (infra vide, see the section “Systemic
Venous Return”), right ventricle filling also changes in
Chapter 36 Effect of Mechanical Ventilation on Heart–Lung Interactions
Changing RV end-diastolic volume changes LV
diastolic compliance
Right ventricle volume (mL)
50
35 20
0
LV Pressure (mm Hg)
20
10
0
0
10
20
30
Left ventricle volume (mL)
40
FIGURE 36-2 Schematic of the effect of increasing right-ventricular
(RV) volumes on the relationship between left-ventricular (LV) diastolic pressure and left ventricle volume (filling). Increases in right
ventricle volumes decrease LV diastolic compliance, such that a higher
filling pressure is required to generate a constant end-diastolic volume.
(Adapted, with permission, from Taylor RR, Covell JW, Sonnenblick
EH, Ross J Jr. Dependence of ventricular distensibility on filling the
opposite ventricle. Am J Physiol. 1967;213:711–718.)
parallel. Increasing RV end-diastolic volume, as occurs during spontaneous inspiration and spontaneous inspiratory
efforts, will reduce LV diastolic compliance, immediately
decreasing LV end-diastolic volume. Positive-pressure ventilation may decrease venous return causing RV volumes
to decrease, increasing LV diastolic compliance. Except in
acute cor pulmonale or biventricular overloaded states, however, the impact of positive-pressure ventilation on LV enddiastolic volume is minimal.
Ventricular interdependence functions through two separate processes. First, increasing RV end-diastolic volume
induces an intraventricular septal shift into the LV, thereby
decreasing LV diastolic compliance (Fig. 36-2).63 Because left
ventricle wall stress is unaltered, any change in LV output
does not reflect a change in LV preload. Because spontaneous inspiration increases venous return, causing right ventricle dilation, LV end-diastolic compliance decreases during
spontaneous inspiration. Whereas right ventricle volumes
usually do not increase during positive-pressure inspiration, ventricular interdependence usually has less impact
over the patient’s hemodynamic status. Second, if pericardial
restraint or absolute cardiac fossal volume restraint limits
absolute biventricular filling, then right ventricle dilation
will increase pericardial pressure, with minimal to no septal shift because the pressure outside of both ventricles will
increase similarly.64,65
Positive-pressure ventilation, however, can still display
right ventricle dilation-associated ventricular interdependence. If positive-pressure inspiration overdistends alveoli,
as for example during lung recruitment maneuvers, pulmonary vascular resistance will increase. Despite the fact that
hemodynamic changes elicited by recruitment maneuvers do
825
not cause persistent cardiovascular insufficiency, transient
right ventricle dilation and left ventricle collapse can occur
during recruitment maneuvers.66 This is an important concept when treating patients with borderline RV failure. Thus,
recruitment maneuvers should be used with caution and be
restricted to 10 seconds or less of an end-inspiratory hold to
avoid significant hemodynamic derangements.
The presence of ventricular interdependence can be
assessed in mechanically ventilated patients based on heart–
lung interactions. Using echocardiographic techniques,
Mitchell et al67 and Jardin et al68 showed that positivepressure breaths decrease RV dimensions, whereas both LV
dimensions and LV flows increase. Still, the changes in RV
output generated by positive-pressure inspiration are much
less than the changes in LV output.69 If ventricular interdependence was the primary process driving hemodynamic
interactions during a positive-pressure breath, then a phasic
increase in LV stroke volume would occur during inspiration. If the primary process was a phasic decrease in venous
return, however, a phasic decrease in LV stroke volume
would be observed two to three beats later, usually during
the expiratory phase, suggesting the right ventricle is preload
responsive. These points underscore the use of LV stroke volume variation during positive-pressure ventilation to identify volume responsiveness.
MECHANICAL HEART–LUNG INTERACTIONS
BECAUSE OF LUNG VOLUME
With inspiration, the expanding lungs compress the heart
in the cardiac fossa,70 increasing juxtacardiac ITP. Because
the chest wall and diaphragm can move away from the
expanding lungs, whereas the heart is trapped within this
cardiac fossa, juxtacardiac ITP usually increases more than
these external ITPs.71,72 This effect is a result of increasing lung volume. It is not affected by the means whereby
lung volume is increased. Both spontaneous73 and positivepressure-induced hyperinflation56,57 induce similar compressive effects on cardiac filling. If one measured only
intraluminal LV pressure, then it would appear as if LV
diastolic compliance was reduced, because the associated
increase in pericardial pressure and ITP would not be
seen.74–76 When LV function, however, is assessed as the
relationship between end-diastolic volume and output, no
evidence for impaired LV contractile function is seen77,74
despite the continued application of PEEP.78 These compressive effects can be considered as analogous to cardiac
tamponade79–81 and are discussed further in the “The Effect
of Intrathoracic Pressure.”
Effect of Intrathoracic Pressure
The heart lives within the thorax, a pressure chamber inside
a pressure chamber. Thus, changes in ITP affect the pressure
gradients for both systemic venous return to the right ventricle and systemic outflow from the left ventricle, independent
826
Part IX
Physiologic Effect of Mechanical Ventilation
Hemodynamic effects of changes in intrathoracic pressure
6
Venous
return
Thorax
LV
Ejection
Blood flow (L/min)
5
B
ITP
4
3
2
Ventricular
function
curve
A
ITP
Venous
return
curve
1
Increasing ITP
Decreases the pressure
gradients for venous
return and LV ejection
Decreasing ITP
Increases the pressure
gradients for venous
return and LV ejection
FIGURE 36-3 Schematic of the effect of increasing or decreasing intrathoracic pressure on the left-ventricular (LV) filling (venous return)
and ejection pressure.
of the heart itself (Fig. 36-3). Increases in ITP, by increasing right-atrial pressure (Pra) and decreasing transmural
LV systolic pressure, will reduce the pressure gradients for
venous return and LV ejection decreasing intrathoracic
blood volume. Using the same argument, decreases in ITP
will augment venous return and impede LV ejection, increasing intrathoracic blood volume. The increases in ITP during
positive-pressure ventilation show marked regional differences; juxtacardiac ITP increases more than lateral chest
wall ITP as inspiratory flow rate and tidal volume increase.71
Interestingly, lung compliance plays a minimal role in defining the positive-pressure-induced increase in ITP. For the
same increase in tidal volume, ITP usually increases similarly if tidal volume is kept constant.82,83 If, however, chest
wall compliance decreases, then ITP will increase for a fixed
tidal volume.84,85
SYSTEMIC VENOUS RETURN
Guyton et al described the determinants of venous return
more than 50 years ago.86,87 Blood flows back from the systemic venous reservoirs into the right atrium through
low-pressure, low-resistance venous conduits. Pra is the
backpressure, or downstream pressure, for venous return.
Pressure in the upstream venous reservoirs is called mean
systemic pressure, and, itself, is a function of blood volume,
peripheral vasomotor tone, and the distribution of blood
within the vasculature.88 Ventilation alters both Pra and
mean systemic pressure. Many of the observed ventilationinduced changes in cardiac performance can be explained by
these changes. Mean systemic pressure does not change rapidly during positive-pressure ventilation, whereas Pra does,
owing to parallel changes in ITP (Fig. 36-4).89,90 Positivepressure inspiration increases both ITP and Pra, decreasing
venous blood flow,35 RV filling, and consequently, RV stroke
volume.35,89–99 During normal spontaneous inspiration, the
opposite effects occur. Spontaneous inspiration decreases
–5
0
5
Right atrial pressure (mm Hg)
10
FIGURE 36-4 A venous return curve, describing the relationship
between the determinants of right-ventricular preload. Right atrial
pressure inversely changes the magnitude of venous return and is influenced by changes in intrathoracic pressure (ITP). Positive-pressure
ventilation shifts the ventricular function curve to the right (A),
increasing right-atrial pressure but decreasing blood flow. Spontaneous
inspiration decreases ITP and shifts the ventricular function curve to
the left (B), decreasing right-atrial pressure but increasing blood flow.
As right-atrial pressure becomes negative, as may occur during forced
inspiratory efforts against resistance or impedance, a maximal blood
flow is reached; further decreases in right-atrial pressure no longer augment venous return.
ITP and Pra, accelerating venous blood flow, and increasing
RV filling and RV stroke volume.35,36,64,93,96,100–102
If changes in Pra were the only process that altered venous
return, then positive-pressure ventilation would induce profound hemodynamic insufficiency in most patients. The
decrease in venous return during positive-pressure ventilation, however, is often lower than one might expect based on
the increase in Pra.
The reasons for this preload-sparing effect seen during
positive-pressure ventilation are twofold. First, when cardiac
output does decrease, increased sympathetic tone decreases
venous capacitance, increasing mean systemic pressure,
which tends to restore the pressure gradient for venous return,
even in the face of an elevated Pra. Increases in sympathetic
tone, however, would increase steady-state cardiac output
and would not alter the phasic changes in venous return
seen during positive-pressure ventilation. The decreased
phasic reductions in venous return are caused by associated increases in mean systemic pressure during inspiration.
Diaphragmatic descent and abdominal-muscle contraction
increase intraabdominal pressure, decreasing intraabdominal vascular capacitance.103,104 Because a large proportion
of venous blood is in the abdomen, the net effect of both
inspiration and PEEP is to increase mean systemic pressure
and Pra in a parallel but unequal fashion.105–107 Accordingly,
the pressure gradient for venous return may not be reduced
as much as predicted as predicted from a pure increase in
Pra. This is an important adaptive response by the body
to positive-pressure ventilation and PEEP, both of which
produce this effect secondary to the associated increase in
lung volume, which promotes diaphragmatic descent. This
Chapter 36 Effect of Mechanical Ventilation on Heart–Lung Interactions
1.0
0.9
0.9
0.8
827
6
4
0.7
0.6
ΔPra
0.5
ΔPaw
ΔPabd
ΔPaw 0.4
2
ΔRVEDV
RVEDV
ΔPaw
0
(%/cm H2O) –2
0.3
0.2
–4
0.1
0
0
–6
FIGURE 36-5 Effect of increasing levels of continuous positive airway pressure (CPAP) on the relations between increasing airway pressure (Paw)
and right-atrial pressure (Pra) (left graph), Paw and intraabdominal pressure (Pabd) (center graph), and Paw and changes in right-ventricular enddiastolic volume (RVEDV) (right graph) in forty-three postoperative fluid-resuscitated cardiac surgery patients. (Data derived, with permission, from
data in Van den Berg P, Jansen JRC, Pinsky MR. The effect of positive-pressure inspiration on venous return in volume loaded post-operative cardiac surgical
patients. J Appl Physiol. 2002;92:1223–1231.)
preload-sparing effect is especially well demonstrated in
patients with hypervolemia. In fact, both the translocation
of blood from the pulmonary to the systemic capacitance
vessels,108 as well as abdominal pressurization secondary to
diaphragmatic descent, may be the major mechanisms by
which the decrease in venous return is minimized during
positive-pressure ventilation.109–113 In fact, van den Berg et
al114 documented that up to 20 cm H2O CPAP did not significantly decrease cardiac output, as measured 30 seconds into
an inspiratory-hold maneuver, in fluid-resuscitated, postoperative cardiac surgery patients. Although CPAP induced
an increase in Pra, intraabdominal pressure also increased,
preventing a significant change in RV volumes (Fig. 36-5).
Interest in inverse-ratio ventilation has raised questions as
to its hemodynamic effect, because its application includes a
large component of hyperinflation.
Current data clearly show that detrimental effects of
increased ITP and PEEP on venous return are far more complex than an effect on the pressure gradient between mean
systemic pressure and Pra, and that geometric deformation
of the venous vasculature and its flow distribution, which
alter the resistance to flow, may be a better explanation.115
Animal data suggest that compression and deformation of
capacitance vessels at the entrance of the thorax103 and compression of the portal circulation by diaphragmatic descent115
may account for these increments in venous resistance and
thus decreased venous return.
Relevance of Intrathoracic Pressure on Venous Return. It
is axiomatic that the heart can only pump out that amount
of blood that it receives and no more. Thus, venous return is
the primary determinant of cardiac output and the two must
be the same.88 Because Pra is the backpressure to venous
return and because Pra is normally close to zero relative
to atmospheric pressure, venous return is maintained near
maximal levels at rest,12,87,94,98,99 because right ventricle
filling occurs with minimal changes in filling pressure.81
Spontaneous inspiratory efforts usually increase venous
return because of the combined decrease in Pra64,94–96,116
and increase in intraabdominal pressure.103,104 For Pra to
remain very low, however, RV diastolic compliance must be
high and RV output must equal venous return. Otherwise,
sustained increases in venous blood flow would distend
the RV and increase Pra. During normal spontaneous
inspiration, although venous return increases, ITP decreases
at the same time, minimizing any potential increase in Pra,
which might otherwise occur if ITP were not to decrease.89
Aiding in this process of minimizing RV workload, the
pulmonary arterial inflow circuit is highly compliant and
can accept large increases in RV stroke volume without
changing pressure.35,117 Thus, increases in venous return
proportionally increase pulmonary arterial inflow without
significant changes in RV filling or ejection pressures.
Accordingly, this compensatory system fails if RV diastolic
compliance decreases or if Pra increases independent
of changes in RV end-diastolic volume. Figure 36-6
illustrates these differential effects of negative (spontaneous
inspiration) and positive (positive-pressure inspiration)
swings in ITP on dynamic RV and LV performance. In RV
failure states, spontaneous inspiration does not decrease Pra
and Pra actually increases. This results in the physical sign
of increased jugular venous distension during spontaneous
inspiration.
Note further in Figure 36-6 that not only does RV stroke
volume increase with spontaneous inspiration and decrease
with positive-pressure inspiration, but also that LV stroke
volume decreases only during spontaneous inspiration
(ventricular interdependence); during positive-pressure inspiration, however, any change in LV stroke volume occurs late, as
the decrease in RV output finally reaches the left ventricle. RV