Overview of Trastuzumab’s Utility for Gastric Cancer pdf
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (278.87 KB, 6 trang )
| Connection 2010
28
Overview of Trastuzumab’s Utility
for Gastric Cancer
Judith Meza-Junco, MD
Heather-Jane Au, MD, FRCPC, MPH
Michael B. Sawyer, MD, BScPhm, FRCPC
Department of Oncology
Cross Cancer Institute
11560 University Avenue
Edmonton, Alberta, Canada, T6G 1Z2
Abstract
Gastric Cancer (GC) is the second leading cause of cancer-related
death worldwide, and has been managed with different treatment
strategies around the world. Surgery is the mainstay of treatment for
non-metastatic disease. Because recurrences are common after curative
resection, adjuvant radio-chemotherapy or perioperative chemotherapy
is recommended. The majority of GC patients in clinical practice have
advanced or metastatic disease, where chemotherapy is considered
standard treatment, to provide palliation and prolong survival; however,
prognosis remains poor. This paper reviews chemotherapy and targeted
therapies for GC, focusing on trastuzumab.
Key Words: Gastric Cancer, HER2, Trastuzumab
Introduction
Gastric cancer (GC) treatment and prognosis vary in different regions
of the world; incidence of the disease, approach to early diagnosis and
treatment varies greatly between western and the eastern hemispheres.
It is the second leading cause of cancer-related death worldwide (1).
In the US, it was estimated there would be 21,500 new cases and
10,880 deaths from GC in 2008; whereas more than 100,000 new
cases are diagnosed and 50,000 die annually of this cancer in Japan.
Approximately 50% of GC cases in Japan are diagnosed at an early
stage, with 5-year survival for stage I GC reported above 90%. In
the Western world only 27% of cases are diagnosed at early stage
and 5-year survival for stage II-III disease is 20-50%, and 5-10% for
stage IV. Different strategies have been tested around the world and
have resulted in different approaches for localized and advanced GC
as summarized in Figure 1.
Chemotherapy for GC
Locoregional and distant recurrences are frequently seen after surgery
for GC, therefore, different approaches as adjuvant and perioperative
therapies have been tested. Three strategies have successfully
demonstrated a survival benefit compared with surgery alone.
Postoperative administration of 5-fluorouracil (5FU) and leucovorin, in
combination with external beam radiation therapy, is routinely used
in the US (2). Perioperative chemotherapy with a combination of
epirubicin, cisplatin and 5FU (ECF), is becoming standard practice
in many countries for resectable GC patients (3). In Japan, adjuvant
monotherapy with surgery + adjuvant chemotherapy (S-1) (Fig. 1) is
common practice (4).
Chemotherapy for advanced unresectable or recurrent GC, in selected
fit patients, offers significant advantages, such as increased survival,
Trastuzumab
Connection 2010 |
29
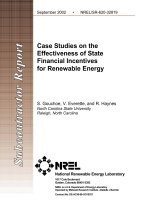
Treatment Options for Gastric Cancer
Localized disease
Advanced disease
Preoperative CT (ECF)
Surgery + Adjuvant CRT(5FU/LV)
Surgery + Adjuvant CT(S-1)
ECF,ECX,DCF
Cisplatin + S1
Irinotecan
CT: chemotherapy; CRT: chemoradiotherapy; ECF: epirubicin, cisplatin, 5FU; ECX: epirubicin, cisplatin, capecitabine;
DCF: docetaxel, cisplatin, 5FU; CT§: chemotherapy with cisplatin and 5FU/capecitabine.
Paclitaxel
Trastuzumab + CT
§
HER2 Positive
Treatment Options for Gastric Cancer
First line therapies
Second line therapies
(No Standard)
symptom control and quality of life, compared to best supportive care
(BSC) alone (5). A recent meta-analysis, showed that chemotherapy
improved overall survival (OS) for 6 months over BSC (Hazard Ratio or
HR of 0.39, 95% Confidence Interval or CI: 0.28-0.52). Best survival rates
were achieved with combined regimens including 5FU, anthracycline,
and cisplatin with a HR of 0.83 (95% CI, 0.74 to 0.93) over single-agent
5FU-based chemotherapy. Response rates (RR) using ECF are 40%,
median survival of 9.4 months and 40% of patients alive at 1 year (6).
Epirubicin, oxaliplatin, and capecitabine (Xeloda
®
) (EOX) combination
treatment has reported a RR of 48%, median survival 11.2 months and
1 year survival of 48% (7).
The DCF regimen (docetaxel, cisplatin, and 5FU) has shown better RR,
longer progression-free survival (PFS) and a small survival advantage
over cisplatin and 5FU (CF) (9.2 vs. 8.6 months; P.02) (8). However,
increased toxicity was seen (such as neutropenic infection and diarrhea),
especially in patients older than 65.
There is no internationally accepted standard of care; monotherapy with
5FU or doublets with 5FU and cisplatin, irinotecan or an anthracycline,
are reasonable alternatives for patients who are not candidates for ECF.
DCF may be recommended as an option in selected very fit patients.
Tegafur (S-1), a 5FU prodrug, is standard therapy for metastatic GC in
Japan; based on a phase III trial. S-1 was not inferior to 5FU in OS, it was
associated with a higher RR, longer PFS, longer time to treatment failure
and longer non-hospitalized survival (9). S-1 has also been compared
to S-1 plus CPT-11, and no differences were seen (10). However, S-1
plus cisplatin showed significantly longer survival over S-1 alone, with
acceptable toxicities.
Figure 1. Treatment options for Gastric Cancer.
Abbreviations: CT: chemotherapy; CRT: chemoradiotherapy; ECF: epirubicin, cisplatin, 5FU; ECX: epirubicin, cisplatin, capecitabine;
DCF: docetaxel, cisplatin, 5FU; CT§: chemotherapy with cisplatin and 5FU/capecitabine
| Connection 2010
30
There is no standard second or third-line of chemotherapy for advanced
GC; less than 40% of patients may be fit for treatment in that setting. One
small phase III study, demonstrated that CPT-11 significantly prolongs
OS (by 50.5 days) and improves tumor related symptoms over BSC (11).
Paclitaxel has showed 20% RR in phase II studies. Molecular targeting
agents are being tested in this setting.
Targeted Therapy for GC
Although there are benefits of palliative chemotherapy, the prognosis of
advanced GC is still poor (median survival 7-10 months). A great interest
in targeted therapies has emerged and several molecular targeting
agents are being tested; including anti-angiogenic agents and epidermal
growth factor receptor (EGFR) antagonists, via monoclonal antibodies
(MAb) (cetuximab, matuzumab, panitumumab and trastuzumab) or
tyrosine kinase inhibitors (TKI) (gefitinib, erlotinib, lapatinib). Matrix
metalloproteinase (MMP), insulin-like growth factor-1 receptor, fibroblast
growth factor, c-Met and downstream signaling inhibitors, as well as
cell cycle associated drugs targets are also under evaluation in phase I
and II studies with advanced GC patients (12, 13). So far, trastuzumab
is the only targeted therapy that has a proven survival benefit in GC.
Table 1 summarizes targeted therapies for GC trials.
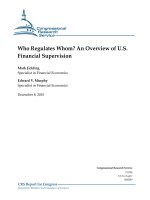
Figure 2.
Anti-tumor effects of Trastuzumab.
Abbreviations: ECD: extracellular domain; VEGF: vascular endothelial growth factor; PI3K: phosphoinositide 3-kinase
Cell Nucleus
HER1, 3 or 4
Breast Cancer Cell
Trastuzumab
Transcription
Amplied number of HER2 genes
on chromosome 17
HER2
Blocks HER2 dimerization blinding to ECD IV
Extracellular eects
Intracellular eects
Activation of antibody dependent cell-mediated
cytotoxicity tumor cell lysis
Receptor down-regulation through
endocytosis
Antiangiogenic eect (HER-family
receptor blockade leads to reductions in
VEGF)
G1 phase arrest
Inhibits signaling
(P13K pathway)
Pro-apoptosis and
proliferation arrest
í
í
í
stop proliferation
Connection 2010 |
31
Drugs and Their Targets Clinical Phase
EGFR antibody:
• Cetuximab
• Panitumumab
• Matuzumab
III
III
I - II
Cetuximab showed RR of 5% in pre-treated patients
Cetuximab + 5FU and oxaliplatin or CPT-11, showed a RR of 44-65% in untreated patients
Cetuximab + docetaxel showed SD in 43% of patients as second line treatment
Matuzumab + ECX showed a DCR of 43-57%
EGFR TKI:
• Getinib
• Erlotinib
II
II
Erlotinib showed a RR of 10% in previously untreated patients
Gefitinib showed SD in 18% of previously treated patients
HER2 antibody:
• Trastuzumab III
Trastuzmab is the only targeted therapy that has a proven survival benefit
VEGFR antibody:
• Bevacizumab III
Phase II studies: bevacizumab with CT (cisplatin and CPT-11; oxaliplatin and docetaxel or 5FU;
DCF) had a RR of 63-71% in untreated patients; but high frequency of toxicity
VEGFR TKI:
• Vatalanib
• Samaxinib
III
Preclinical
FGFR TKI:
• Brivanib
• Ki23057
II
Preclinical
IGF-R antibody:
• CP-751,871
IGF-R TKI:
• OSI 906
I - II
I
HGF/Met-R antibody:
• AMG 102
HGF/Met-R TKI:
• GSK1363089 (XL880)
• Arqule
I - II
II
I - II
Dual TKI EGF/HER2-R:
• Lapatinib
Dual TKI EGF/VEGF-R:
• Vadetenib
II
Preclinical
Lapatinib showed a DCR of 25% in previously untreated patients
Multi TKI (Raf, VEGFR-2, VEGFR-3, PDGFR-β:
• Sorafenib
Multi TKI (RET, VEGFR, PDGFR, Flt3, c-KIT):
• Sunitinib
II
II
Sunitinib showed a DCR of 40%
Sumilar efficacy was observed with sorafenib combined with docetaxel and cisplatin.
Table 1. Targeted Therapies for Advanced Gastric Cancer.
Abbreviations: RR: response rate; SD: stable disease; PR: partial response; CR: complete response; DCR: diease control rate (SD, PR, CR); CT: chemotherapy;
ECX: epirubicin, cisplatin, capecitabine; DCF: docetaxel, cisplatin, 5FU
| Connection 2010
32
Trastuzumab
HER2/neu and Trastuzumab
HER2/neu (c-erbB-2) is a transmembrane tyrosine kinase (TK) receptor,
member of the human epidermal growth factor-receptor (HER) family
(HER1, 2, 3 and 4). HER2 function and signaling activity requires
receptor dimerization followed by transactivation of the TK portion of the
dimer. Phosphorylation allows recruitment and activation of downstream
proteins, and the signaling cascade is initiated. Given HER2 functions
as an oncogene, gene amplification induces protein over-expression in
cell membranes and regulates signal transduction in cellular processes,
such as proliferation, differentiation, and cell survival. Aberrant HER2
expression or function has been associated in carcinogenesis of breast,
gastric, ovarian, salivary gland, prostate and lung tumors (14).
Trastuzumab is a recombinant humanized anti-HER2 MAb (rhuMAb
HER2; molecular weight 145531.5 g/mol), directed against the HER2
extracelluar domain (ECD). It was engineered from a cloned human
IgG, with structure and antigen-binding residues of a potent murine
MAb 4D5. The antibody was humanized to minimize the immunogenicity
associated with murine MAb and to enhance endogenous immune
antitumor effects (Fig. 2). Its exact mechanism is not completely known,
however extracellular and intracellular actions have been postulated:
Extracellular Mechanisms:
Blocks HER2 receptor cleavage and inhibits dimerization,
consequently reducing HER2 signaling.
By endocytosis, increases receptor destruction. Trastuzumab
seems to induce HER2 down regulation and subsequent
degradation in HER2 over-expressing cancer cells.
Intracellular Mechanisms:
Inhibits intracellular signaling pathways, such as
phosphoinositide 3-kinase (PI3K) signaling.
Has anti-angiogenesis effect through decreasing vascular
endothelial growth factor (VEGF) produced by tumor cells; it
may indirectly modulate proangiogenic and antiangiogenic
factors, as well as synergistic activity with chemotherapy.
Facilitates G1 phase arrest, by inducing cyclin-dependent
kinase (CDK) inhibitor p27Kip1.
Has Cytostatic and Cytotoxic activity due to immune
system recruitment by antibody-dependent cell-mediated
cytotoxicity (ADCC).
Trastuzumab Tolerability
Trastuzumab is generally well tolerated. The most common side effects
are infusion-related reactions (fever, rigors, chills, nausea, dyspnea
and hypotension), which may be present in 40% of patients with the
first dose, and 5% with subsequent administrations. Myelosuppression,
nausea and emesis are rare and alopecia has not been reported
when trastuzumab is used alone; however, when it is given with
chemotherapy, it is difficult to quantify its contributions to these effects.
Cardiotoxicity (impairment of left ventricular ejection fraction) was
evident in 27% of patients treated with trastuzumab and anthracyclines,
13% with trastuzumab and paclitaxel, and 5% with trastuzumab alone
in a pivotal study in breast cancer.
Post-marketing surveillance reported that 62 of 25,000 (0.002%)
patients had serious adverse events due to trastuzumab, including
hypersensitivity reactions, infusion-related reactions and pulmonary
events. Adult respiratory distress syndrome, anaphylaxis, and death
within 24 hours of a trastuzumab infusion were reported; most of these
occurred in patients with preexisting pulmonary dysfunction (15).
Trastuzumab Efficacy in GC
Over-expression and amplification of HER2/ErbB2 in GC varies widely
(6-45%). The largest data set of 3,883 advanced GC samples,
found HER2-positivity rates of 22.9%; immunohistochemical (IHC) and
fluorescence in situ hybridization (FISH) concordance was 87.3%.
No differences were seen between European and Asian countries.
HER2-positivity was higher in intestinal than diffuse/mixed cancer
(32.2 vs. 6.1%/20.4%; p<0.001) and in gastro-esophageal junction
cancers than GC (33.2 vs. 20.9%; p<0.001) (16).
Early studies in GC cell lines which over-expressed HER2 showed growth
inhibition by trastuzumab; when it was combined with doxorubicin,
cisplatin or paclitaxel it demonstrated increased cytotoxicity (17).
A small phase II study including 21 advanced GC patients with
“
Trastuzumab in combination with
chemotherapy is a reasonable treatment
option for patients with HER2-positive
advanced GC, although this includes
only approximately 20% of patients as
potential candidates.
”
Connection 2010 |
33
over-expression/amplification of HER2; showed that (18) after
trastuzumab treatment (8 mg/kg loading dose in the first cycle followed
by 6 mg/kg every 21 days) and cisplatin (75 mg/m
2
every 21 days),
response rates were 35% and stable disease was 17%. The therapy was
well tolerated and no grade 4 toxicities were seen.
The first randomized, controlled phase III trial, (ToGA) evaluated
trastuzumab efficacy and safety in HER2-positive advanced GC. Patients
were randomized to receive trastuzumab with 5FU or capecitabine and
cisplatin versus chemotherapy alone. Preliminary results showed better
median survival with the combination (13.5 vs. 11.1 month, p=0.0048;
HR 0.74; 95% CI 0.60, 0.91), with a 26% reduction in risk of death. PFS
was 6.7 vs. 5.5 months (p=0002); and disease control (DC) was 47.3%
vs. 34.5% (p=0.0017) with the addition of trastuzumab vs. chemotherapy
alone. Toxicity profiles were similar in both groups. Subgroup analysis
(site of tumor, performance status, fluoropyrimidine used, histology,
age, region, prior gastrectomy and number of metastatic sites) for
survival favored trastuzumab throughout. Additionally, patients with high
HER2-positivity by IHC had a trend for better survival in the pre-planned
analysis; patients with HER2 IHC2+/FISH+ or IHC3+ had a longer
survival (16 months) with trastuzumab compared to chemotherapy alone
(11.8 months) (19).
Conclusion
Prognosis of GC remains poor even after advances in diagnostics,
surgical techniques, chemotherapy and radiotherapy regimens, thus,
novel treatment options and predictors of treatment response are
needed. Advanced or metastatic GC constitutes most of patients seen in
western clinical practice. For them, chemotherapy has been considered
standard with significant advantages (increased survival, symptom
control and quality of life) compared to BSC alone. Trastuzumab is the
only targeted therapy that has now shown in a randomized trial modest
but clinically significant improvement in survival, with no increases in
toxicity, for patients with a poor prognosis. Trastuzumab in combination
with chemotherapy is a reasonable treatment option for patients with
HER2-positive advanced GC, although this includes only approximately
20% of patients as potential candidates.
Further investigation are required to evaluate trastuzumab’s efficacy for
advanced GC as monotherapy, maintenance treatment after doublet or
triplet regimens, in continuation beyond progression, and in combination
with second line therapy; as well, in curative treatment trials for GC
patients, such as peri-operative or postoperative therapy.
Glossary
Curative resection: Complete tumor resection with
negative surgical margins.
Adjuvant radio-chemotherapy: Combination of
radiotherapy and chemotherapy given after a radical
treatment (e.g., surgery), to destroy undetectable
residual tumor cells.
Perioperative chemotherapy: Chemotherapy given
before and after surgery.
Hazard ratio: is the effect of a variable (e.g., treatment)
on the risk of an event (e.g., survival); it is considered an
estimate of relative risk.
References
1. Sugano K. Gastric cancer: pathogenesis, screening
and treatment. Gastrointest. Endocopy Clin N Am 2008;
18:513-22.
2. Macdonald JS, Smalley SR, Benedetti J, et al.
Chemoradiotherapy after surgery compared with
surgery alone for adenocarcinoma of the stomach
or gastroesophageal junction. N Engl J Med 2001;
345:725-30.
3. Cunningham D, Allum WH, Stenning SP, et al. MAGIC
Trial Participants. Perioperative chemotherapy versus
surgery alone for resectable gastroesophageal cancer.
N Engl J Med 2006; 355:11-20.
4. Sakuramoto S, Sasako M, Yamaguchi T, et al. ACTS-
GC Group. Adjuvant chemotherapy for gastric cancer
with S-1, an oral fluoropyrimidine. N Engl J Med 2007;
357:1810-20.
5. Wagner AD, Grothe W, Haerting J, et al. Chemotherapy
in advanced gastric cancer: a systematic review and
meta-analysis based on aggregate data. J Clin Oncol
2006; 24:2903-9.
6. Ross P, Nicolson M, Cunningham D, et al. Prospective
randomized trial comparing mitomycin, cisplatin, and
protracted venous-infusion fluorouracil (PVI 5-FU)
with epirubicin, cisplatin, and PVI 5-FU in advanced
esophagogastric cancer. J Clin Oncol 2002;
20:1996-2004.
7. Cunningham D, Starling N, Rao S, et al. Upper
Gastrointestinal Clinical Studies Group of the
National Cancer Research Institute of the United
Kingdom. Capecitabine and oxaliplatin for advanced
esophagogastric cancer. N Engl J Med 2008; 358:36-46.
8. Van Cutsen E, Moiseyenko VM, Tjulandin S, et al.
Phase III study of docetaxel and cisplatin plus fluorouracil
compared with cisplatin and fluorouracil as first-line
therapy for advanced gastric cancer: A Report of the
V325 Study Group. J Clin Oncol 2006; 24:4991-7.
9. Boku N, Yamamoto S, Shirao K, et al. Randomized
phase III study of 5-fluorouracil (5-FU) alone versus
combination of irinotecan and cisplatin (CP) versus S-1
alone in advanced gastric cancer (JCOG9912). Annual
meeting of ASCO 2007; (aLBA4513T).
10. Imamura H, IIishi H, Tsuburaya A, et al. Randomized
phase III study of irinotecan plus S-1 (IRIS) versus S-1
alone as first-line treatment for advanced gastric cancer
(GC0301/TOP-002). ASCO Gastrointestinal Symposium
2008; (a5).
11. Wilson D, Hiller L, Geh JI. Review of second-line
chemotherapy for advanced gastric adenocarcinoma.
Clin Oncol (R Coll Radiol) 2005; 17:81-90.
12. Arkenau HT. Gastric cancer in the era of molecularly
targeted agents: current drug development strategies.
J Cancer Res Clin Oncol 2009; 135:855-66.
13. Meza-Junco J, Au HJ, Sawyer MB. Trastuzumab for
gastric cancer. Expert Opin Biol Ther 2009; 9:1543-51.
14. Hudis CA. Trastuzumab – mechanism of action and use
in clinical practice. N Engl J Med 2007; 357:39-51.
15. González V, Salgueiro E, Jimeno FJ, et al. Post-marketing
safety of antineoplasic MAb: rituximab and trastuzumab.
Pharmacoepidemiol Drug Saf 2008; 17:714-21.
16. Bang Y, Chung H, Xu J, et al. Pathological features of
advanced gastric cancer (GC): Relationship to human
epidermal growth factor receptor 2 (HER2) positivity in
the global screening programme of the ToGA trial. J Clin
Oncol 2009; 27:15S (a4556).
17. Gong SJ, Jin CJ, Rha SY, et al. Growth inhibitory effects
of trastuzumab and chemotherapeutic drugs in gastric
cancer cell lines. Cancer Lett 2004; 214:215-24.
18. Cortés-Funes H, Rivera F, Alés I, et al. Phase II of
trastuzumab and cisplatin in patients (pts) with advanced
gastric cancer (AGC) with HER2/neu over-expression/
amplification. 2007 ASCO Annual Meeting Proceedings,
J Clin Oncol 2007; 25:18s (a4613).
19. Van Cutsem E, Kang Y, Chung H, et al. Efficacy results
from the ToGA trial: A phase III study of trastuzumab
added to standard chemotherapy (CT) in first-line human
epidermal growth factor receptor 2 (HER2)-positive
advanced gastric cancer (GC). J Clin Oncol 2009;
27:18s(aLBA4509).