Pediatric emergency medicine trisk 356
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (173.27 KB, 4 trang )
Marker to patient’s
head
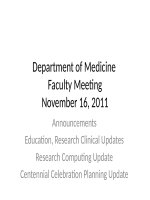
Cardiac
Pericardial
effusion
a For
Low-frequency
Anechoic fluid in Pericardiocentesis
probe
the pericardial
space between
Subxiphoid,
the pericardium
marker to
and
patient’s right
myocardium,
Parasternal long,
tracks anterior to
marker to
descending aorta
patient’s left hip
in parasternal
long view
details, see Chapter 131 Ultrasound .
SUMMARY
Respiratory distress is one of the most common chief complaints of children
seeking medical care. History and physical examination provides important clues
that allow rapid localization of the site of impairment. The underlying cause must
be identified and may be within the respiratory system or organ systems that
control or impact respiration. Any disorder that causes respiratory distress may be
life threatening. Airway and ventilatory problems not only must be recognized
but also must be anticipated and addressed aggressively. The underlying cause
must also be treated. Patients must be monitored continuously and reassessed
frequently. Airway, breathing, and circulation must be established and
maintained. Diagnostic evaluation of body fluids, radiologic studies, direct
visualization, and specialized tests of organ function must be performed prudently
so that respiratory status is not further compromised.
Suggested Readings and Key References
Cherry JD. Clinical practice. Croup. N Engl J Med 2008;358(4):384–391.
de Caen AR, Berg MD, Chameides L, et al. Part 12: Pediatric advanced life
support: 2015 American Heart Association Guidelines Update for
cardiopulmonary resuscitation and emergency cardiovascular care. Circulation
2015;132(18 Suppl 2):S526–S542.
Gadomski AM, Permutt T, Stanton B. Correcting respiratory rate for the presence
of fever. J Clin Epidemiol 1994;47(9):1043–1049.
Hammer J. Acute respiratory failure in children. Paediatr Respir Rev
2013;14(2):64–69.
King C, Henretig FM, King BR, et al., eds. Textbook of pediatric emergency
procedures . 2nd ed. Baltimore, MD: Williams & Wilkins; 2007:85–251, 383–
409, 823–901.
Krauss BS, Harakal T, Fleisher GR. The spectrum and frequency of illness
presenting to a pediatric emergency department. Pediatr Emerg Care
1991;7(2);67–71.
Louie MC, Bradin S. Foreign body ingestion and aspiration. Pediatr Rev
2009;30(8):295–301.
McIntosh K. Community-acquired pneumonia in children. N Engl J Med
2002;346(6):429–437.
Miller EK, Gebretsadik T, Carroll KN, et al. Viral etiologies of infant
bronchiolitis, croup and upper respiratory illness during 4 consecutive years.
Pediatr Infect Dis J 2013;32(9):950–955.
O’Dempsey TJ, Laurence BE, McArdle TF, et al. The effect of temperature
reduction on respiratory rate in febrile illnesses. Arch Dis Child
1993;68(4):492–495.
Pfleger A, Eber E. Management of acute severe upper airway obstruction in
children. Paediatr Respir Rev 2013;14(2):70–77.
Ralston SL, Lieberthal AS, Meissner HC, et al. Clinical practice guideline: the
diagnosis, management, and prevention of bronchiolitis. Pediatrics
2014;134(5):e1474–e1502.
Shah SN, Bachur RG, Simel DL, et al. Does this child have pneumonia?: the
rational clinical examination systematic review. JAMA 2017;318(5):462–471.
Tibballs J, Watson T. Symptoms and signs differentiating croup and epiglottitis. J
Paediatr Child Health 2011;47(3):77–82.
CHAPTER 72 ■ SEIZURES
AMIR A. KIMIA, VINCENT W. CHIANG
Seizures are the clinical expression of abnormal, excessive, synchronous
discharges of neurons residing primarily in the cerebral cortex. This paroxysmal
activity is intermittent and its duration may last from a few seconds to many
hours. Seizures represent a neurologic emergency either due to the underlying
cause (e.g., bleed, infection) or the potential for neuronal death as a result of a
prolonged seizure. Approximately 5% of children will have at least one seizure in
the first 16 years of life. The immature brain, particularly in the neonate and
young infant, differs from the adult brain in the basic mechanisms of
epileptogenesis and propagation of seizures. It is more prone to seizures, but
seizures are also more apt to disappear as the child grows. Physicians must have a
fundamental knowledge of seizure classification (semiology), all aspects of
seizure management (including initial stabilization), determination of cause
(differential diagnosis), appropriate definitive treatment, and patient disposition.
BACKGROUND
A seizure is defined as a transient, involuntary alteration of consciousness,
behavior, motor activity, sensation, and/or autonomic function caused by an
excessive rate and hypersynchrony of discharges from a group of cerebral
neurons. A convulsion is a seizure with prominent alterations of motor activity.
Epilepsy, or seizure disorder, is a condition of susceptibility to recurrent seizures.
Seizures may be generalized or partial. Generalized seizures reflect
involvement of both cerebral hemispheres. These may be convulsive or
nonconvulsive. Consciousness may be impaired and this impairment may be the
initial manifestation. Motor involvement is bilateral. Types of generalized
seizures include absence (petit mal), myoclonic, tonic, clonic, atonic, and tonicclonic (grand mal) seizures.
Partial (focal, local) seizures reflect initial involvement limited to one cerebral
hemisphere. Partial seizures are further classified on the basis of whether
consciousness is impaired. When consciousness is not impaired, the seizure is
classified as a simple partial seizure. Simple partial seizures may have motor,
somatosensory/sensory, autonomic, or psychic symptoms. When consciousness is
impaired, the seizure is classified as a complex partial seizure. Both simple and
complex partial seizures may evolve into generalized seizures (Jacksonian
spread). The spread to deep subcortical regions and evolution to a bilateral tonic-
clonic seizure is now called bilateral tonic-clonic seizure (previously referred to
as a secondarily generalized seizure), to differentiate it from seizures that are
generalized from the onset.
It is important to recognize that generalized seizures with focal manifestations
are also considered focal. These manifestations may include lateral eye deviation,
head tilt, postictal Todd paresis (or paralysis), or psychomotor seizures (also
referred to as temporal lobe seizures).
Status epilepticus is a form of prolonged seizure. This is defined as seizures
lasting more than 5 minutes or repetitive seizure activity without recovery of
consciousness in between episodes. This is an operational definition used to guide
therapy. While only 25% of pediatric seizures last longer than 5 minutes, the
longer a seizure persists, the more difficult it becomes to control. If a child is seen
in the ED with a reported/witnessed generalized seizure that has resolved, a 30minute cutoff is used to define status, because 30 minutes is when the risk of
permanent neuronal injury increases significantly. Status epilepticus is the highest
form of seizure emergency.
A postictal (decreased responsiveness) period usually follows a seizure. During
this time, the patient may be confused, lethargic, fatigued, or irritable; also,
headache, vomiting, and muscle soreness may occur. In general, the length of the
postictal period is proportional to the length of the seizure. For brief seizures,
there may be few or no postictal symptoms. Transient focal deficits (e.g., Todd
paralysis) may occur during the postictal period, but one must first rule out a
focal central nervous system (CNS) deficit.
PATHOPHYSIOLOGY
The underlying abnormality in all seizures is the hypersynchrony of neuronal
discharges. Cerebral manifestations include increased blood flow, increased
oxygen and glucose consumption, and increased carbon dioxide and lactic acid
production. If a patient can maintain appropriate oxygenation and ventilation, the
increase in cerebral blood flow is usually sufficient to meet the initial increased
metabolic requirements of the brain. Brief seizures rarely produce any lasting
effects.
Multiple animal studies and a recent study in humans indicate that 30 minutes
of generalized convulsive status epilepticus increases the risk of permanent
neuronal injury.
Systemic alterations may occur with seizures and result from a massive
sympathetic discharge, leading to tachycardia, hypertension, and initially stress
hyperglycemia. Failure of adequate ventilation, especially in patients in whom