Báo cáo y học: " An adult case of urinary tract infection with Kingella kingae: a case report" doc
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (803.58 KB, 3 trang )
Case report
Open Access
An adult case of urinary tract infection with Kingella kingae:
a case report
KV Ramana* and SK Mohanty
Address: Department of Microbiology, Kamineni Institute of Medical Sciences (KIMS), Narketpally, Nalgonda-508254, India
Email: KVR -
* Corresponding author
Published: 11 May 2009 Received: 22 February 2008
Accepted: 22 January 2009
Journal of Medical Case Reports 2009, 3:7236 doi: 10.1186/1752-1947-3-7236
This article is available from: />© 2009 Ramana and Mohanty; licensee Cases Network Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (
/>which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction: Kingella kingae, though part of the normal upper respiratory tract and genitourinary
tract, is increasingly being recognized as an important human pathogen. During the past decade, it has
emerged as a significant pathogen in the pediatric age group primarily causing bacteremia and
osteoarticular infections. Adult infection usually occurs in individuals who are severely
immunocompromised and most infections have taken the form of septicemia or septic arthritis.
Bacteremia due to K. kingae has been reported as the immediate cause of death in patients with
acquired immunodeficiency syndrome.
Case presentation: We present a microbiologically confirmed urinary tract infection with K. kingae
in an immunocompetent 45-year-old adult woman with post-menopausal bleeding and with a history
of clots. Her urine was subjected to culture and sensitivity tests. The isolated colonies were identified
as K. kingae because of their typical culture characteristics such as long incubation period required for
growth, beta-hemolysis, positive oxidase and negative catalase, urease indole, nitrate and citrate tests.
Penicillin G disc test was positive. They were sensitive to all conventional antibiotics.
Conclusion: K. kingae infection is a rare occurrence in immunocompetent adults. Very few cases of
microbiologically confirmed infections have been reported so far. The isolation of K. kingae from
urine sample has rarely been reported. K. kingae isolates are either missed or misinterpreted by
clinical microbiologists. Therefore, K. kingae deserves recognition as a pathogen.
Introduction
In 1976, Moraxella kingae was removed from the genus
Moraxella and was given a new genus and species name
Kingella kingae in the family Neisseriaceae [1]. Besides
K. kingae, other species belonging to the genus Kingella are
K. denitrificans, K. indolegenes and K. oralis. K. kingae
exhibits a variable morphology (cocci, short Gram-
negative coccobacilli to medium sized rods) and is
considered to be a normal flora of the upper respiratory
tract and genitourinary tract [2]. It has been associated
with infections in children under 6 years and immuno-
compromised individuals [2].
Page 1 of 3
(page number not for citation purposes)
Poor oral hygiene, pharyngitis and mucosal ulceration are
the predisposing factors for K. kingae infections [2,3].
K. kingae bacteremia without endocarditis has also been
reported in immunocompetent adults following dental
manipulations [4]. K. kingae has specific tissue tropism for
cardiac, valvular, joint space, and skeletal tissue and has
been isolated from cases of bacteremia, endocarditis, bone
and joint infection in various samples such as blood, joint
fluid, and urine [5].
We report an adult patient with urinary tract infection
from whom K. kingae has been isolated in urine.
Case presentation
A 45-year-old woman was admitted to the gynaecology
ward of Kamineni Institute of Medical Sciences Hospital,
Narketpally complaining of post-menopausal bleeding
with passing of clots for the previous 18 months. She also
complained of burning micturition.
Urine was sent for culture and sensitivity tests. It was
turbid and routine urine microscopic examination
revealed the presence of 5 to 8 pus cells per high power
field. Urine was inoculated in blood agar, MacConkey’s
agar and incubated at 37°C. Overnight incubation showed
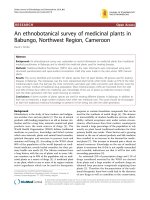
no growth. A pure growth of 1 mm round, convex
b-hemolytic colonies was observed on blood agar after
48 hours of incubation, with no growth on MacConkey’s
agar (Figure 1). Gram stain of the isolated colonies
showed varied morphology (cocci, diplococci, coccoba-
cilli) (Figure 2). They were non-motile, oxidase-positive
but were negative for catalase (Moraxella and Neisseria were
positive), indole (K. indolegenes was positive), citrate,
urease, and nitrate (K. denitrificans was positive). Only
glucose and maltose (K. oralis was also positive for
sucrose) were fermented. The Gram stained smear of the
first subculture from blood agar showed short Gram-
negative bacilli (Figure 3). Simultaneously, the Penicillin
G disc test [6] was performed and revealed Gram-negative
plump, elongated rods (Neisseria were negative) (Figure
4). The isolated colonies were found to be susceptible to
penicillin (10 µg), ampicillin (25 µg), oxacillin (1 µg),
gentamicin (30 µg), amikacin (30 µg), TMP-SMX (25 µg),
cefotaxime (30 µg), ceftriaxone (30 µg), norfloxacin (10
µg), netilmicin (30 µg) and nalidixic acid (30 µg). The
isolated organism was identified as K. kingae because of its
fastidious nature, slow growth, b-hemolysis, varied Gram
morphology, oxidase positivity, catalase negativity and
positive penicillin G disc test.
Discussion
K. kingae, though a part of the normal upper respiratory
tract and genitourinary tract, is increasingly being recog-
nized as an important human pathogen. During the past
decade, it has emerged as a significant pathogen in the
pediatric age group primarily causing bacteremia and
osteoarticular infections [7,8]. Adult infection usually
occurs in individuals who are severely immunocompro-
mised and most infections have taken the form of
septicemia or septic arthritis. Bacteremia due to K. kingae
has been reported as the immediate cause of death in
patients with acquire d immunodeficienc y syndrome
(AIDS) [2].
K. kingae infection is a rare occurrence in immunocompe-
tent adults. Very few cases of microbiologically confirmed
infections have been reported so far [9]. The isolation of
K. kingae from urine samples has rarely been reported [6].
Figure 1. Growth on Blood agar after 48 hours of aerobic
incubation showing pinpoint translucent haemolytic colonies.
Figure 2. Gram stain picture on day one showing
Gram-negative cocci & coccobacilli.
Page 2 of 3
(page number not for citation purposes)
Journal of Medical Case Reports 2009, 3:7236 />We isolated K. kingae from the urine of an immunocom-
petent 45-year-old woman with post-menopausal bleed-
ing and with clots for the previous 18 months. In this
patient, the possible source of K. kingae was the resident
genital flora. Due to the regular flow of clots and tissue, the
organism could have gained access through the urethra
causing ascending urinary tract infection. Kingellae are
nutritionally fastidious Gram-negative bacilli requiring
48 hours of incubation before reaching a colony size of 1
mm diameter. They are oxidase-positive, catalase-negative
(Moraxella are positive) and positive for the Penicillin G
disc test. Of all of the species, K. kingae is b-hemolytic on
sheep blood agar [2]. The isolation of K. kingae is often
either missed or misinterpreted. Cases of K. kingae
infection are on the rise in children as well as in
immunocompromised and immunoco mpetent a dults.
Therefore, K. kingae deserves recognition as a pathogen.
Abbreviations
AIDS, acquired immunodeficiency syndrome.
Consent
Written informed consent was obtained from the patient
for publication of this case report and any accompanying
images. A copy of the written consent is available for
review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
KVR analyzed and interpreted the patient data regarding
the urine culture. SKM was a major contributor in writing
the manuscript. Both authors read and approved the final
manuscript.
Acknowledgements
We acknowledge the support of all teaching and technical
staff at Kamineni Institute of Medical Sciences.
References
1. Henriksen SD, Bovre K: Transfer of Moraxella kingae Henriksen
and Bøvre to the genus Kingella gen. nov. in the family
Niesseriaceae. Int J Syst Bacteriol 1976, 26:447-450.
2. Winn WC, Allen S, Janda WM, Koneman EW, Schreckenberger PC,
Procop G, Baker Woods G. Miscellaneous fastidious Gram-
negative bacilli.InKoneman’s Color Atlas and Textbook of Diagnostic
Microbiology.6
th
edition. Philadelphia, PA, Lippincott, Williams and
Wilkins; 2006:472-473.
3. Shimeld LA, Rodgers AT. Essentials of Diagnostic Microbiology. Clifton
Park, NY, Delmar Learning; 1999:180.
4. Roiz MP, Peralta FG, Arjona R: Kingella kingae bacteremia in an
immunocompetent adult host. J Clin Microbiol 1997, 35:1916.
5. Manuselis G, Barnishan J. Haemophilus species, HACEK group,
Pasteurella, Brucella, Francicella species.InTextbook of
Diagnostic Microbiology.2
nd
edition. Edited by Mahon CR,
Manuselis G. Philadelphia, PA, Saunders; 2000:440.
6. Long KS, Thomas JG, Barnishan J. Neisseria species and Moraxella
catarrahlis.InTextbook of Diagnostic Microbiology.2
nd
edition. Edited
by Mahon CR, Manuselis G. Philadelphia, PA, Saunders; 2000:408.
7. Yagupsky P, Dagan R: Kingella kingae: An emerging cause of
invasive infections in young children. Clin Infect Dis 1997,
24:860-866.
8. Yagupsky P, Dagan R, Howard CW, Einhorn M, Kassis I, Simu A: High
prevalence of Kingella kingae in joint fluid from children with
septic arthritis revealed by the BACTEC blood culture
system. J Clin Microbiol 1992, 30:1278-1281.
9. Van Damme PA, Van Harpen CM, Meis JF: An adult case of oral
infection with Kingella kingae. Int J Oral Maxillofac Surg 2004,
33(1):105-107.
Figure 3. Gram stain picture of first subculture showing
Gram-negative bacilli.
Figure 4. Gram stain picture of colonies grown in the
presence of penicillin (Penicillin G disc test) showing elongated
Gram-negative bacilli.
Page 3 of 3
(page number not for citation purposes)
Journal of Medical Case Reports 2009, 3:7236 />