Thuốc chống viêm: chọn lọc các chất ức chế ppt
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (105.77 KB, 4 trang )
Vol 10, No 2, March/April 2002
75
The nonsteroidal anti-inflammatory drugs (NSAIDs)
generally possess anti-inflammatory, analgesic, and
antipyretic activity. All of these medications have
some adverse effects, but the most frequently associat-
ed adverse effect with NSAIDs is gastrointestinal (GI)
toxicity, a source of both morbidity and mortality,
especially with prolonged usage in the elderly. Risk
factors for the development of NSAID-induced gastric
problems include individuals aged >60 years, history
of GI ulcer or bleeding, concomitant use of cortico-
steroids or anticoagulants, higher NSAID doses, and
serious systemic illnesses. The incidence of GI toxicity
is 20 to 40 per 1,000 patient-years of exposure.
1
Renal,
platelet, and central nervous system toxicity also have
been observed. Although no currently available
NSAID lacks GI toxicity, specific cyclooxygenase-2
(COX-2) inhibition appears to be an improvement over
conventional NSAIDs. The selective COX-2 inhibitor
celecoxib was approved for use in the United States by
the FDA in 1998 to treat osteoarthritis and rheumatoid
arthritis. Rofecoxib was approved in 1999 for osteo-
arthritis, acute pain, and primary dysmenorrhea.
Currently, additional agents, such as a parenteral form,
parecoxib, and its active metabolite, valdecoxib, are
under development.
Structure and Mechanism of Action
The anti-inflammatory effect of NSAIDs is due mainly
to the inhibition of the COX enzymes, which are
required for the synthesis of prostaglandins and throm-
boxanes. The recycled oxygenases are biofunctional
hemoproteins that catalyze the oxygenation of arachi-
donic acid to prostaglandin, a common precursor for
the synthesis of the family of prostaglandins, prostacy-
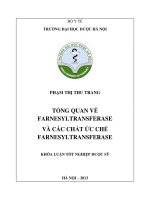
cline and thromboxanes. Two COX isoforms exist that
catalyze the same reaction but are different in terms of
regulation and expression (Fig. 1). COX-1, which is
expressed constitutively in most tissues, is thought to
protect the gastric mucosa and maintains renal homeo-
stasis and normal platelet function. COX-2 is expressed
constitutively in the brain and the kidney but can be
induced in other tissues and at sites of inflammation.
The discovery of a second isoform of COX established
the rationale for the development of specific COX-2
inhibitors as a novel class of anti-inflammatory com-
pounds as compared with current NSAIDs, which inhibit
both COX-1 and COX-2 to a similar degree. Clinical
trials have shown that a specific COX-2 inhibitor can
achieve therapeutic efficacy in osteoarthritis and pain
management while avoiding the serious side effects, in
particular GI ulceration, dyspepsia, and bleeding, related
to the COX-1 inhibition observed with the general
NSAIDs. The COX-2 inhibitors are effective because the
side chain on these drugs fits well into the COX-2 enzy-
matic pocket but is too large to fit into the COX-1 enzy-
matic pocket. In humans, therapeutic concentrations of
the COX-2 inhibitors (coxibs) celecoxib and rofecoxib do
not significantly inhibit the COX-1 isoenzyme.
Pharmacokinetics
Celecoxib is rapidly absorbed, reaching peak serum
concentrations in about 3 hours. The drug is metabo-
lized in the liver by CYP2CP (a cytochrome P-450 isoen-
zyme) into carboxylic acid and glucuronide metabolites
and excreted in feces and urine. It has a half-life of
about 11 hours. Rofecoxib, which is metabolized in the
liver by cytosolic enzymes, reaches maximum concen-
tration within 2 hours and has an effective half-life of
approximately 17 hours. With the ingestion of a fatty
meal, the absorption of celecoxib is increased 10% to
20%, and the time to peak concentration for both drugs
is delayed 1 to 2 hours. With the use of nonprescription
antacids there is a decrease in the area under the plasma
concentration curve, and thus the rate of absorption of
Dr. Lane is Chief, Metabolic Bone Disease Service, and Medical Director, Os-
teoporosis Prevention Center, Hospital for Special Surgery, New York, NY.
The author or the department with which he is affiliated has received
something of value from a commercial or other party related directly or
indirectly to the subject of this article.
Reprint requests: Dr. Lane, 535 East 70th Street, New York, NY 10021.
Copyright 2002 by the American Academy of Orthopaedic Surgeons.
J Am Acad Orthop Surg 2002;10:75-78
Anti-inflammatory Medications: Selective COX-2 Inhibitors
Joseph M. Lane, MD
Advances in Therapeutics and Diagnostics
both coxibs may be prolonged; but this effect should not
be of clinical significance in the long-term treatment of
arthritis. Elderly patients (aged >65 years) may exhibit
a decrease of up to 30%, but this does not mandate a
dose adjustment.
Indications for Use
Celecoxib has been shown to achieve a significant re-
duction in joint pain compared with placebo.
4,5
Celecoxib was evaluated for treatment of the signs and
symptoms of osteoarthritis of the knee and hip in
approximately 4,200 patients in placebo- and active-con-
trolled clinical trials of 12 weeks’ duration. In patients
with osteoarthritis, treatment with celecoxib 100 or 200
mg qd resulted in a significant improvement as mea-
sured by the Western Ontario and McMaster University
(WOMAC) index, a composite of pain, stiffness, and
functional measures in osteoarthritis. In three 12-week
studies of pain accompanying osteoarthritis flare, cele-
coxib doses of 100 and 200 mg bid provided notable
reduction in pain within 24 to 48 hours of initiation of dos-
ing. At doses of 100 mg or 200 mg bid, the effectiveness of
celecoxib was similar to that of naproxen 500 mg bid.
Doses of 200 mg bid provided no additional benefit over
100 mg bid. A total daily dose of 200 mg is equally ef-
fective whether administered as 100 mg bid or 200 mg qd.
Celecoxib has demonstrated significant (P < 0.05)
reduction in rheumatoid arthritis in joint tenderness,
pain, and joint swelling compared with placebo. It was
evaluated for treatment of the signs and symptoms of
rheumatoid arthritis in approximately 2,100 patients in
placebo- and active-controlled clinical trials of up to 24
weeks’ duration. Celecoxib was shown to be superior to
placebo as measured by the ACR20 Responder Index, a
composite of clinical, laboratory, and functional mea-
sures in rheumatoid arthritis. Doses of 100 and 200 mg
bid were similar in effectiveness, and both were compa-
rable to the effectiveness of naproxen 500 mg bid.
Although celecoxib 100 and 200 mg bid provided similar
overall effectiveness, some patients derived additional
benefit from the 200 mg bid dose. Doses >200 mg bid
provided no additional benefit above that seen with 100
to 200 mg bid.
Rofecoxib has demonstrated significant (P < 0.001)
reduction in joint pain of osteoarthritis compared with
placebo.
6,7
The signs and symptoms of osteoarthritis of
the knee and hip were assessed in placebo- and active-
controlled clinical trials of 6 to 86 weeks’ duration that
enrolled approximately 3,900 patients. In patients with
osteoarthritis, treatment with rofecoxib 12.5 and 25 mg
qd resulted in improvement in patient and physician
global assessments and in the WOMAC osteoarthritis
questionnaire, including pain, stiffness, and functional
measures of osteoarthritis. In six studies of pain accom-
panying osteoarthritis flare, rofecoxib provided a signif-
icant (P < 0.05) reduction in pain at the first determina-
tion (after 1 week in one study, after 2 weeks in the
remaining five studies); this continued for the duration
of the studies. In all of the osteoarthritis clinical studies,
once-daily treatment in the morning with rofecoxib 12.5
and 25 mg was associated with a significant (P < 0.05)
reduction in joint stiffness on first awakening in the
morning. At doses of 12.5 and 25 mg, the effectiveness
of rofecoxib was shown to be comparable to that of
ibuprofen 800 mg tid and diclofenac 50 mg tid for
osteoarthritis. The ibuprofen studies were 6-week stud-
ies; the diclofenac studies were 12-month studies in
which patients could receive additional arthritis med-
ication during the last 6 months.
In acute analgesic models
8-10
of postoperative dental
pain, postorthopaedic surgical pain, and primary dys-
menorrhea, rofecoxib relieved pain rated by patients as
moderate to severe. The analgesic effect (including onset
of action) of a single 50-mg dose was generally similar
to that of naproxen 550 mg or ibuprofen 400 mg. In a
single-dose postoperative dental pain study, the onset of
analgesia with a single 50-mg dose occurred within 45
minutes. In a multiple-dose study of postorthopaedic
surgical pain in which patients received rofecoxib or
placebo for up to 5 days, 50 mg qd was effective in
reducing pain. In this study, patients on rofecoxib con-
sumed a significantly smaller amount of additional anal-
gesic medication than did patients treated with placebo
(1.5 versus 2.5 doses per day of additional analgesic
medication for rofecoxib and placebo, respectively).
In a randomized, placebo- and active-comparator-
controlled clinical trial using a postoperative dental pain
model, 272 patients with moderate to severe pain ran-
Selective COX-2 Inhibitors
Journal of the American Academy of Orthopaedic Surgeons
76
(−)
Glucorticoids
(−)
NSAIDs
Physiologic stimulus Inflammatory stimulus
COX-1
Constitutive
Platelets
Endothelium
Stomach
Mucosa
Intestines
Kidney Brain Kidney
COX-2
Constitutive Inducible
Macrophages
Synoviocytes
Endothelial cells
Figure 1 The distribution, regulation, and function of COX-1 and
COX-2. The black boxes indicate drug interventions that inhibit
the pathway. (Adapted with permission.
2,3
)
domly received a single dose of placebo, rofecoxib 50
mg, celecoxib 200 mg, or ibuprofen 400 mg.
8
Overall
analgesic effect, time to onset, peak effect, and duration
of effect were assessed. Rofecoxib was significantly (P <
0.001) more effective than celecoxib and placebo in all
measures of analgesic efficacy. Rofecoxib and ibuprofen
had similar time to onset and time to confirmed percep-
tible pain relief (approximately 30 minutes compared
with 1 hour for celecoxib); there were no measurable
effects for placebo. In addition, rofecoxib had a longer
duration of action compared with median time to use of
rescue medication: approximately 5 hours for celecoxib,
10 hours for ibuprofen, and >24 hours for rofecoxib.
Valdecoxib also has been shown to be efficacious as
an opioid-sparing analgesic in patients undergoing total
hip arthroplasty. Patients receiving either 20 or 40 mg of
valdecoxib bid for 48 hours after total hip arthroplasty
required 40% less morphine than did those in control
groups.
11
Other uses of NSAIDs, such as in the preven-
tion of heterotopic ossification, have not been tested with
COX-2 inhibitors.
Drug Interactions and Adverse Effects
Because rofecoxib is not metabolized by the cytochrome
P450 pathway, it has fewer confirmed drug interactions.
However, potent inducers of cytochrome oxidase, such
as rifampin, may decrease rofecoxib concentrations sim-
ply by increasing hepatic metabolism in general. Clini-
cal studies with celecoxib have identified potentially
important interactions with fluconazole and lithium,
making careful patient monitoring mandatory. Similar
to other NSAIDs, rofecoxib has the potential to interact
with furosemide and with angiotensin-converting
enzyme inhibitors. These agents may interact with war-
farin; thus, coagulation studies should be monitored
after initiating celecoxib or rofecoxib. Rofecoxib is asso-
ciated with an 8% increase in the international normal-
ized ratio (INR).
The most common effects of COX-2 inhibitors have
been abdominal pain, diarrhea, and dyspepsia.
4,12
Both
coxibs have been evaluated through endoscopic studies.
Over a 12-week period, duodenal ulcers occurred in 7%
of patients treated with celecoxib 200 mg bid, compared
with 10% treated with diclofenac 75 mg bid, 35% with
naproxen 500 mg bid, 23% with ibuprofen 800 mg tid,
and 4% given a placebo. In another treatment study, the
cumulative incidence of ulcers at 12 weeks was 9.9% in
patients treated with placebo, 4.1% in those given rofe-
coxib 25 mg qd, 7.3% in those given rofecoxib 50 mg qd,
and 27% in those given ibuprofen 2,400 mg qd or 800
mg tid. Thus, both agents are associated with a notable
decline in GI irritation.
Unlike other NSAIDs, celecoxib and rofecoxib do not
inhibit platelet aggregation or increase bleeding time.
However, in a study in which aspirin in any dosage was
an exclusion criterion, the risk of myocardial infarction
was five times higher in the rofecoxib than in the na-
proxen group (0.5% versus 0.1%, respectively; P < 0.05).
13
In a study in which 22% of patients received low-dose
aspirin therapy, rates of myocardial infarction were not
different between the two groups; however, similarly,
there was no difference in the rate of significant perfora-
tion or bleeding unless the group taking aspirin was
excluded from the study.
12
Differences in cardiovascu-
lar results between the two trials may represent trial
design and chance or differences in the specific pharma-
cology of the various COX-2 inhibitors.
14
These issues
question the need for the concurrent use of low-dose
aspirin in appropriate patients and the resultant effec-
tiveness of the COX-2 inhibitors in diminishing GI toxic-
ity in that setting.
Both coxibs may lead to a significant (P < 0.02) rise in
systolic blood pressure in 10% to 17% of patients, greater
with rofecoxib.
15
Fluid retention and edema have been
observed in some patients (5% celecoxib, 10% rofecoxib).
COX-2 inhibitors should not be given to patients with
aspirin-induced asthma. Celecoxib is contraindicated in
patients with known allergic reaction to sulfonamide.
Although other NSAIDs that inhibit COX-1 and
COX-2 taken in the postoperative period may have a
deleterious effect on achieving spinal fusion, there are
no such data for the coxibs. However, an animal
model study demonstrated that a specific COX-2 in-
hibitor more effectively blocked lamellar bone forma-
tion elicited by strain than did indomethacin.
16
COX-2
inhibitors in a rat femoral fracture model resulted in a
65% nonunion rate compared with 18% in the NSAID
group and 0% in the control group. The animals also
had greater angulation and a poorer histologic score,
suggesting that COX-2 inhibitors should be used with
caution in humans when bone healing is required.
17
Dosage and Cost
Celecoxib is available in 100- and 200-mg tablets (Table 1).
The recommended dose for osteoarthritis is 200 mg qd or
100 mg bid and for rheumatoid arthritis, 100 to 200 mg bid.
Rofecoxib is available in 12.5-, 25-, and 50-mg tablets.
The recommended dose for osteoarthritis is 12.5 mg qd.
Some patients may receive additional benefit by increas-
ing the dose to 25 mg qd. For acute pain and treatment
of primary dysmenorrhea, the recommended dose is 50
mg qd with subsequent doses of 50 mg qd as needed.
Use for more than 5 days to manage pain has not been
studied. Both coxibs may be taken with or without food.
Joseph M. Lane, MD
Vol 10, No 2, March/April 2002
77
Summary
Celecoxib and rofecoxib appear to be as effective as the
conventional NSAIDs for the treatment of osteoarthritis.
Celecoxib is also labeled for rheumatoid arthritis and
rofecoxib for acute pain. Both may also be effective for
short-term pain relief. The safety profile of the COX-2
inhibitors appears to be superior to that of the other
NSAIDs and their efficacy, comparable. However, there
is an apparently increased rate of myocardial infarction
and the loss of the gastroprotective advantage in
patients who also must take daily aspirin. Therefore,
what is the current role of these agents with reference to
other NSAIDs? The patient who has had a previously
favorable result with or is currently using a standard
NSAID can be maintained on that agent. If the patient
previously had a GI toxicity, then use of a COX-2
inhibitor would be appropriate. For the patient who has
not taken NSAIDs and has any of the risk factors out-
lined above for GI side effects, use of a COX-2 inhibitor
is indicated. For those without any risk factors, the pro-
jected length of administration (short course versus
chronic use), cost, and relative risks and benefits can be
discussed with the patient. In summary, these agents
appear to offer an improved safety profile compared
with the classic NSAIDs, and where bleeding or indi-
gestion is an issue, they are the drugs of choice.
Selective COX-2 Inhibitors
Journal of the American Academy of Orthopaedic Surgeons
78
References
1. MacDonald TM, Morant SV, Robinson GC, et al: Association
of upper gastrointestinal toxicity of non-steroidal anti-inflam-
matory drugs with continued exposure: Cohort study. BMJ
1997;315:1333-1337.
2. Garnett WR: Clinical implications of drug interactions with
coxibs. Pharmacotherapy 2001;21:1223-1232.
3. Verburg KM, Maziasz TJ, Weiner E, Loose L, Geis GS, Isakson
PC: COX-2-specific inhibitors: Definition of a new therapeutic
concept. Am J Ther 2001;8:49-64.
4. Bensen WG, Fiechtner JJ, McMillen JI, et al: Treatment of
osteoarthritis with celecoxib, a cyclooxygenase-2 inhibitor: A
randomized controlled trial. Mayo Clin Proc 1999;74:1095-1105.
5. Williams GW, Hubbard RC, Yu SS, Zhao W, Geis GS: Com-
parison of once-daily and twice-daily administration of cele-
coxib for the treatment of osteoarthritis of the knee. Clin Ther
2001;23:213-227.
6. Cannon GW, Caldwell JR, Holt P, et al: Rofecoxib, a specific
inhibitor of cyclooxygenase 2, with clinical efficacy compara-
ble with that of diclofenac sodium: Results of a one-year, ran-
domized, clinical trial in patients with osteoarthritis of the
knee and hip: Rofecoxib Phase III Protocol 035 Study Group.
Arthritis Rheum 2000;43;978-987.
7. Day R, Morrison B, Luza A, et al: A randomized trial of the
efficacy and tolerability of the COX-2 inhibitor rofecoxib vs
ibuprofen in patients with osteoarthritis: Rofecoxib/Ibuprofen
Comparator Study Group. Arch Intern Med 2000;160:1781-1787.
8. Malmstrom K, Daniels S, Kotey P, Seidenberg BC, Desjardins
PJ: Comparison of rofecoxib and celecoxib, two cyclooxyge-
nase-2 inhibitors, in postoperative dental pain: A randomized,
placebo- and active-comparator-controlled clinical trial. Clin
Ther 1999;21:1653-1663.
9. Morrison BW, Daniels SE, Kotey P, Cantu N, Seidenberg B:
Rofecoxib, a specific cyclooxygenase-2 inhibitor, in primary
dysmenorrhea: A randomized controlled trial. Obstet Gynecol
1999;94:504-508.
10. Reicin A, Brown J, Jove M, et al: Efficacy of single-dose and
multidose rofecoxib in the treatment of post-orthopedic
surgery pain. Am J Orthop 2001;30:40-48.
11. Camu F, Beecher T, Recker DP, Verburg KM: Valdecoxib, a
COX-2-specific inhibitor, is an efficacious, opioid-sparing anal-
gesic in patients undergoing hip arthroplasty. Am J Ther
2002;9:43-51.
12. Silverstein FE, Faich G, Goldstein JL, et al: Gastrointestinal
toxicity with celecoxib vs nonsteroidal anti-inflammatory
drugs for osteoarthritis and rheumatoid arthritis: The CLASS
study: A randomized controlled trial: Celecoxib Long-term
Arthritis Safety Study. JAMA 2000;284:1247-1255.
13. Bombardier C, Laine L, Reicin A, et al: Comparison of upper
gastrointestinal toxicity of rofecoxib and naproxen in patients
with rheumatoid arthritis: VIGOR Study Group. N Engl J Med
2000;343:1520-1528.
14. FitzGerald GA, Cheng Y, Austin S: COX-2 inhibitors and the
cardiovascular system. Clin Exp Rheumatol 2001;19(6 suppl
25):S31-S36.
15. Whelton A, Fort JG, Puma JA, et al: Cyclooxygenase-2–specif-
ic inhibitors and cardiorenal function: A randomized, con-
trolled trial of celecoxib and rofecoxib in older hypertensive
osteoarthritis patients. Am J Ther 2001;8:85-95.
16. Forwood MR: Inducible cyclo-oxygenase (COX-2) mediates
the induction of bone formation by mechanical loading in
vivo. J Bone Miner Res 1996;11:1688-1693.
17. Leonelli S, Goldberg B, Safanda J, Bagwe M, King S,
Sethuratnam S: Abstract: The effect of cyclooxygenase 2 (COX-
2) inhibitors on bone healing. Trans Orthop Res Soc 2002;27:65.
Table 1
Cost Comparison of Coxibs and NSAIDs
Drug Usual Dosage Cost
*
Celecoxib 100 mg bid $84.95
200 mg qd $71.73
Rofecoxib 25 mg qd $73.29
Generic diclofenac 150 mg bid $26.83
Voltaren 150 mg bid $100.50
Generic naproxen 500 mg bid $17.93
Naprosyn 500 mg bid $90.28
Generic ibuprofen 800 mg tid $11.45
Motrin 800 mg tid $38.15
*
Cost for 30 days’ treatment on www.drugstore.com. Accessed
August 2001.