đánh giá hiệu quả của xạ trị kết hợp capecitabine trước mổ trong ung thư trực tràng thấp tiến triển tại chỗ bản tóm tắt tiếng anh
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (275.46 KB, 24 trang )
1
ABBREVIATIONS
AJCC American Joint Commitee on Cancer
BN Patient
BTV Biological target volume
CLVT Computed Tomography
GĐ Stage
GTV Gross tumor volume
HT Chemotherapy
HXT Chemoradiotherapy
HMMD Immunohistochemistry
HMNT Ostomy
IGRT Image guided radiation therapy
IMRT Intensity modulated radiation therapy
IQR Interquartile range
M Metastasis
MBH Pathology
MRI Magnetic resonance imaging
N Lymph nodes
NCCN National Comprehensive Cancer Network
PET/CT Positron emission tomography/computed tomography
PT Surgical
RHM Anal margin
SUV max Standardized Uptake Value maximum
T Tumor
cTNM clinical TNM
pTNM pathological TNM
TRG Tumor regression grade
TT Rectum
XT Radiation
UTBM Adenocarcinoma
UTĐTT Colorectal cancer
UTTT Rectal cancer
WHO World Health Organization
INTRODUCTION
1. Scientific aims
2
Colorectal cancer is one of the common cancers in our country and around
the world. The incidence of this cancer is increasing. In developed countries,
colorectal cancer ranks the second most common cancer, after lung cancer in men
and breast cancer in women. In France, each year there are about 34,500 cases of
colorectal cancer and approximately 16,800 deaths. In the United States, there is
about 41,000 new cases every year, 6-13% of new patients with stage T4 disease.
Approximately 5-30% of these patients will have recurrence.
In Vietnam, colorectal cancer is among common cancers and ranks sixth in
all cancers, with the incidence of 9.2/100,000 population and the mortality rate of
5.0/100,000 population. Currently, almost rectal cancer patients present with late-
stage disease, and the lesions have invaded the surrounding tissues. Due to this, the
rate of radical and anal preserving surgery is low, particularly when the tumor has
invaded in the sacrum (T4). Therefore, survival and quality of life is not high. In
recent years, locally advanced rectal cancer patients have been treated by
preoperative radiotherapy. But there are still cases resistant to radiation (Vo Van
Xuan: The rate of complete response after preoperative radiotherapy: 8.9%). The
proportion of palliative care patients with ostomy was high (according to Vo Quoc
Hung: 21.5%).
In the world today, the treatment of rectal cancer is progressing and
changing. Many authors are researching new techniques, medications and
coordinating methods in order to improve the efficiency of treatment and quality of
life. One of these is preoperative radiochemotherapy. There have been some studies
using capecitabine plus preoperative radiotherapy (45 to 50.4 Gy) for locally
advanced rectal cancer patients. These studies showed positive results: down-stage,
increased the rate of anal sphincter-preserving surgery (Elwanis et al, 2009: down-
stage after radiochemotherapy was 74.4%)
In Vietnam until now there have been no studies about this issue, specifically
assessing the effectiveness of preoperative radiochemotherapy for locally advanced
rectal cancer patients (T3, T4). Therefore, we are undertaking this study:
"Evaluating the effects of preoperative radiochemotherapy with Capecitabine in
low locally advanced rectal cancer"
2. Objectives
2.1. Evaluating the effectiveness of preoperative radiochemotherapy with
Capecitabine in low locally advanced rectal cancer
2.2. Assessing the side effects of this regime
3. The contributions of the thesis
- Confirmed the role and effectiveness of Capecitabine combined with
preoperative radiotherapy in low locally advanced rectal cancer. The
functional response: 100%; response rate 90.8%; complete response: 9.2%; the
down-stage: 46.0%. The tumor volume expended to rectal circumference
was decreased after treatment. Before treatment: 52.9% of patients with
tumors expanded entire circumference and this dropped 16.1% after
treatment. 2.3% of patients tumors had a complete response after treatment.
40.0% of patients fell over 10,000 mm3 tumor volume on 1.5Tesla magnetic
3
resonance image. 40.2% of patients had before treatment CEA levels >
5ng/ml, of these patients 91.4% had reduced levels of CEA after treatment.
79.3% of patients were operated, in which 67.8% had radical surgery and
12.6% underwent anal sphincter-preserving surgery. 9.2% of patients had
recurrence or metastasis and 11.5% of patients died in the follow-up of 36
months.
- Assessed the haematological, hepatic and renal toxicities of this regimen:
preoperative radiation plus Capecitabine in low locally advanced rectal cancer: low
toxicities, mostly grade 1 and 2.
- Evaluated the gastrointestinal, urinary tract and skin complications of this
regimen. The majority of patients had undesirable effects with low rates at grade 1
and 2 (nausea, vomiting, stomatitis, diarrhea): 23.0%, 20.7%, 1.1%; 5.7%,
respectively, 39.1% of patients had red inflamed skin in the radiated area, 12.6%
had ulcers in irradiated skin, 32.2% of patients had cystitis and 24.1% of patients
had pain in the anus.
4. The structure of the thesis
The thesis consists of 121 pages, with 4 main chapters: Introduction 2 pages,
Chapter 1 (Overview) 32 pages, Chapter 2 (Patients and Methods) 18 pages, Chapter 3
(results) 33 pages, Chapter 4 (discussion) 32 pages, Conclusion and recommendation 3
pages.
The thesis has 39 tables, 23 pictures, 12 diagrams, 126 references (30
Vietnamese, 95 English and 1 French).
CHAPTER 1: OVERVIEW
1.1. Anatomy of rectum
1.2. Diagnostic workup
1.2.1. Signs and symptoms
1.2.2. Tests
1.2.3. Staging: according to AJCC: American Joint Committee on Cancer 2010
1.3. Treatment of rectal cancer
1.3.1. Surgery in rectal cancer
1.3.2. Radiation therapy in rectal cancer
Preoperative radiation: helps reduce the size of the tumor, contributes to making
surgery easier, increases the rate of radical and anal sphincter-preserving surgery.
Some studies showed that preoperative radiotherapy reduces the 50% risk of local
recurrence which significantly increases survival. Preoperative radiotherapy doses
of 45Gy-50.4Gy in 5 weeks are being studied, becoming a more and more popular
trend in reseach. Preoperative radiotherapy is indicated for locally advanced rectal
cancer (stage T3, T4)
1.3.3. Chemotherapy in rectal cancer
Radiochemotherapy: Recent researches shows that 5FU is an attractive
radiosensitizer. Radiochemotherapy is indicated for locally advanced rectal cancer
(stage T3, T4), N(-/+). So far, many studies about preoperative radiochemotherapy
4
for rectal cancer found the positive results included down-stage, reduced local
recurrence and increased survival.
Chemotherapy options and doses for concomitant chemotherapy during radiation:
1. 5FU 325-350mg/m
2
+ Leucovorin 20mg/m
2
IV, bolus, d1-5, week 1 and 5
2. 5FU 400mg/m
2
+ Leucovorin 100mg/m
2
IV, bolus, d1,2,11,12,21,22
3. 5FU 1000mg/m
2
IV, bolus, d1-5, week 1 and 5
4. 5FU 250mg/m
2
IV continuous infusion on days 1-14 and 22-35 and
Oxaliplatin 50mg/m
2
IV d1,8,22,29
5. 5FU 225mg/m
2
continuous infusion 5 days per week, together with
radiotherapy
6. Capecitabine 800-825mg/m
2
, bid po continuously, 5-7 days per week,
together with radiotherapy
7. UFT 300-350mg/m
2
/day and Leucovorin 22,5-90mg/day po continuously, 5-
7 days per week, together with radiotherapy
1.4. Chemotherapy drug information used in research
1.5. Previous studies about preoperative radiochemotherapy in rectal cancer
1.5.1. Foreign studies:
Kim JS et al (2002): Primary tumor and node downstaging occurred in 63%
and 90% of patients, respectively. The overall downstaging rate, including both
primary tumor and nodes, was 84%. A pathologic complete response was achieved
in 31% of patients. Twenty-one patients had tumors located initially 5 cm or less
from the anal verge; among the 18 treated with surgery, 72% received sphincter-
preserving surgery. No Grade 3 or 4 hematologic toxicities developed. Other Grade
3 toxicities were as follows: hand-foot syndrome (7%), fatigue (4%), diarrhea (4%),
and radiation dermatitis (2%). Kim JC et al (2005): Downstaging rate was 71%
(56/79) on endorectal ultrasonography, and it was 76% (71/94) on pathology
finding. No tumor cell was observed in the specimens of 11 patients (12%). 40
patients (74%) underwent sphincter-preserving procedures. Grade 3 toxicities were
rare (diarrhea in 3% and neutropenia in 1%). Elwanis et al (2009): Preoperative
chemoradiation resulted in a complete pathologic response in 4 patients (9.3%) and
an overall downstaging in 32 patients (74.4%). Sphincter sparing surgical
procedures were done in 20 out of 43 patients (46.5%). Toxicity was moderate and
required no treatment interruption. Grade II anemia occurred in 4 patients (9.3%),
leukopenia in 2 patients (4.7%) and radiation dermatitis in 4 patients (9.3%)
respectively. Valentini V. et al (2009): 100 patients were included. R0 resection
was performed in 78 patients. R0 resection rate was greater in females (93% vs
67%) and in responders to neoadjuvant chemoradiation (94% vs 60%). The ability
to perform a sphincter-saving procedure was 57%, greater in middle rectal location.
1.5.2. Vietnamese studies:
In Vietnam, radiation for rectal cancer was applied from the 1980s, only
using preoperative Cobalt radiotherapy with doses of 36Gy. Since 2000, linear
accelerators have been installed in Vietnam and have been used to treat rectal
cancer.
Đoàn Hữu Nghị (1994): preoperative radiotherapy is effective in reducing
5
pain (71.1%), decreased sensation tenesmus and reduce the number patients of
bloody diarrhea (63.5%) in majority of cases. Author Pham Quoc Dat (2002): the
average survival following preoperative radiation therapy was 70 months, after
radiotherapy before and after surgery was 46.5 months and using radiotherapy
postoperatively was 36 months. Vo Quoc Hung (2004) reviewed some of the
clinical features and histology and evaluated the response of preoperative
radiotherapy in rectal cancer at Hospital K with doses of 36Gy and 45Gy. This
showed that 100% patients had improved functional symptoms, 41.0% patients had
reduced tumor size ≥ 50%, 51.8% patients had tumor change from fixed to mobile
after radiotherapy. Complications of preoperative radiotherapy include: perineal
pain 83.9%, cystitis 33.9%, 16.9% digestive disorders, ulcers and cirrhosis on the
irradiated area 8.9% and 7.1% intestinal adhesion. The rate of radical surgery was
78.5%, in which 21.4% had conservation surgery. Radiation therapy with a dose of
45Gy was better than 36Gy. Author Vo Van Xuan (2012) studied 56 rectal cancer
patients treated by preoperative hyperfractionated radiation showed the complete
response rate was 8.9%, partial response rate was 73.2%; entire response rate was
82.1%. Miles surgery was 48.2%, 10.7% Hartmann surgery, sphincter-preserving
surgery: 23.2%; ostomies surgery: 17.9%.
The studies of foreign authors showed that preoperative radiochemotherapy
(Capecitabine + Radiation) for locally advanced rectal cancer patients had good results
and increased the rate of radical and sphincter-preserving surgery. The response rate of
radiochemotherapy is better than radiotherapy alone, less toxicity. In Vietnam, the T3,
T4 stage rectal cancer patients were treated by preoperative radiation therapy but the
results were not high. To update the new treatments to be similar to new regimens in
the world, we undertook this study to evaluate the effectiveness of preoperative
radiochemotherapy for locally advanced rectal cancer patients.
Chapter 2: PATIENTS AND METHODS
2.1. Patients
87 patients with stage 3, 4 low rectal cancer treated by preoperative
radiochemotherapy at The Center of Nuclear Medicine and Oncology, Bach Mai
Hospital and Department of Radiation 4, K Hospital from 6/2009 to 12/2012
2.1.1. Patient criteria:
- Patients diagnosed with low rectal cancer (tumors located ≤ 6 cm from the anal
margin): it was histopathological adenocarcinoma, ring cell carcinoma, mucinous
carcinoma, tumor was fixed or limited mobile, with or without lymph node
metastasis, no distant metastasis.
- Age ≤ 85; The patients must have Karnofsky > 60% or 1 - 2 ECOG score (Eastern
Cooperative Oncology Group)
- Good function of bone marrow, kidney and liver
- Patients who do not suffer from other acute and chronic severe diseases.
2.1.2. Exclusion criteria of patients:
- Patients diagnosed:
+ High, middle rectal cancer (tumors located > 6cm from the anal margin)
6
+ Tumor was mobile (stage 1,2 according to Y.Mason)
+ Distant metastasis
- Anal cancer: squamous cell carcinoma developed from skin and anal mucosa of
external anus, inguinal lymph node metastasis.
- Age > 85; The patients have Karnofsky ≤ 60% or 3-4 ECOG score
2.2. Methods:
2.2.1. Research design:
The method was clinical intervention study without control
p
p
Zn
.
1
2
2
)2/1(
ε
α
−
=
−
The sample size was calculated by the formula:
2.2.2. Steps
Patients who had the criteria will be selected in the study. Patient’ medical records
were made in the standard form. Data collection selected by medical research form
2.2.2.1. Clinical and test characteristics before treatment:
* Clinical characteristics
* Subclinical characteristics
+ Colonoscopy
+ Pelvic MRI
+ Tests to evaluate the state of distant metastasis
+ CBC tests
+ Blood biochemical tests
+ Histology tests
2.2.2.2. Treatment plan:
- All low rectal cancer patients with criteria received preoperative concurrent
chemoradiotherapy:
Chemotherapy: Oral Capecitabine (Xeloda) 825mg/m2 twice daily on
radiotherapy days (5days/week), drug manufactured by Hoffmann-La Roche
Radiation:
• Radiotherapy technique: using a linear accelerator with three-dimensional
technique (3D conformal)
• Energy: 6 MeV and 15 MeV
• Using CT simulation for planning treatment
• Patients posture: prone, straight legs, two hands over head, fasting before
radiotherapy.
• The volume of radiation: tumor and lymph nodes and around the rectum
location where tumor spreads
• Beam: three or four beams
• Using lead for shielding normal tissues (dose of radiation on the tumor and
lymph nodes is maximal but the healthy surrounding organs is minimal)
• Dose Radiation: Total dose: 46Gy/25 fractions, 200cGy/day, 5 days/week
2.2.2.3. Assess the effects of research
+ Subjective response: Evaluate response based on the functional symptoms,
7
patient’s answere on questions about: bloody diarrhea, frequency of defecation,
tenesmus feeling, before and after treatment, compared on each with other of
patients
+ Objective response:
* Criteria for evaluation the response treatment after preoperative radiotherapy
based on RECIST (Response Evaluation Criteria in Solid tumors):
• Complete Response: Disappearance of all target lesions
• Partial Response: At least a 30% decrease in the sum of the longest diameter
of target lesions, taking as reference the baseline sum longest diameter
• Stable Disease: Neither sufficient shrinkage to qualify for Partial Response
nor sufficient increase to qualify for Progressive Disease, taking as reference
the smallest sum longest diameter since the treatment started
• Progressive Disease: At least a 20% increase in the sum of the longest
diameter of target lesions, taking as reference the smallest sum longest
diameter recorded since the treatment started or the appearance of one or
more new lesions
* Criteria for evaluation of tumor response:
+ Evaluate Response based on rectal examination before and after treatment:
* Evaluate response based on compared tumor size and mobility
* Based on compared the tumor volume with rectal circumference before and after
treatment
* Based on the down- stage according to Y. Mason classification
+ Assessing Response based on pelvic 1.5 Tesla MRI before and after
treatment:
* Evaluate response based on compared pelvic MRI before and after treatment on
each patient: rate of down-stage
* Evaluate response based on compared tumor volume before and after treatment
on each patient with tumors were cubic form. Assessed by pelvic 1.5 Tesla MRI:
the formula of tumor volume used: Volume = length × width × height × 0.52
• The change of tumor volume on MRI: tumor volume before treatment -
tumor volume after treatment
• The percentage of tumor reduced volume after treatment: = (tumor volume
before treatment - tumor volume after treatment) x100/the tumor volume
before treatment
• Compared the value of tumor volume before and after treatment with Paired-
Samples T Test
* Assess tumor stage and lymph nodes before and after treatment by pelvic 1.5
Tesla MRI with TNM classification of AJCC 2010
+ Assess Response by comparing CEA levels before and after treatment:
* Assess based on compared CEA before and after treatment in each patient with
CEA pre-treatment levels > 5ng/ml:
• Assess by CEA before and after treatment: CEA level before treatment -
CEA level after treatment
• The average percentage of decreased CEA levels after treatment: (CEA
8
before treatment-after treatment)x100/CEA before treatment
• Compare CEA levels before and after treatment: by Paired-Samples T Test
+ Assess Response based on the rate of surgery:
* After radiation treatment, patients were evaluated response, noted side effects.
Surgery was usually done after 3 weeks of radiation therapy.
* Evaluate the rate of radical, anal sphincter-preserving surgery, after
chemoradiotherapy and assessing tumor and lymph nodes stage after surgery (pT,
pN) according to the TNM classification of AJCC 2010
+ Assess Response based on histopathology after surgery:
- Assess the rate of cell degeneration
- Assess tumor regression grade (TRG) by Dworak et al:
+ TRG 0: No regression: Fibrosis was completely absent
+ TRG 1: Minor regression: Dominant tumor mass with obvious fibrosis in 25% or
less of the tumor mass
+ TRG 2: Moderate regression: Dominant tumor mass with obvious fibrosis in 26% to
50% of the tumor mass
+ TRG 3: Good regression: Dominant fibrosis outgrowing the tumor mass; more
than 50% tumor regression
+ TRG 4: Total regression: No viable tumor cells; only fibrotic mass
- Evaluate the fibrosis around the tumor
- Assess of mucosal tank
- The phenomenon of fatty macrophage
- The phenomenon of hemoglobin macrophages
- The phenomenon epithelial regenerated reaction
- The phenomenon slipped and ulcerated epithelium
- The phenomenon of degenerative intestinal wall
Divided the patients into two groups:
Response: include complete response and partial response
No response: include stable disease and progressive disease
* Review the relationship between response with some factors such as age, sex,
stage of disease, histological type, pretreatment CEA levels
* Review the relationship between the tumor regression with some factors such as
age, sex, stage of disease, histological type, pretreatment CEA levels
+ In case of progressive disease after radiochemotherapy, patients treated by
radiation and chemotherapy or ostomies surgery
2.2.2.4. Assess the side effects (toxicities): according to WHO Common Toxicity
Criteria for Anticancer Drugs and the Common Terminology Criteria for Adverse
Events Version 4.0 (CTCAE) of National Cancer Institute 2009
2.3. STASTICS
* The information is encoded and processed by SPSS 16.0 software
* The statistical algorithms: description, comparative tests
CHAPTER 3: RESULTS
9
3.2. Evaluate Response:
3.2.1. Functional response:
Table 3.1. The rate of post-treatment functional response
Functional response n %
The percentage of response,
patients identified (all symptoms)
< 50% 12 13,8
≥ 50%
75 86,2
Total 87 100
3.2.2. Evaluate Response based on rectal examination and rectoscopy before
and after treatment:
Figu
re 3.1. The tumor volume with rectal circumference (RCC)
10
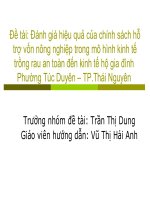
Figure 3.2. Changing stage after treatment
3.2.3. Assessing Response based on pelvic 1.5Tesla MRI:
Table 3.2. Changing the tumor volume before and after treatment on MRI
Changing the tumor volume before and after treatment (mm3) n %
Increased 2 5,7
Decreased 0-1000 0 0
Decreased 1001-5000 8 22,9
Decreased 5001-10000 11 31,4
Decreased 10001-20000 6 17,1
Decreased > 20000 8 22,9
Total 35 100
The percent of average tumor volume decreased after treatment: 78,9 ± 17,3%
11
The percent of average tumor volume reduced (in 33 patients had decreased tumor
volume): 25606,12 mm
3
3.2.4. Assess Response by comparing CEA levels
Table 3.3. CEA levels before and after treatment
CEA levels (ng/ml)
Before treatment After treatment
n % n %
≤ 5 52 59,8 64 73,6
5,01-10 11 12,6 12 13,8
10,01-15 9 10,3 2 2,3
15,01-20 2 2,3 4 4,6
>20 13 15,0 5 5,7
Total 87 100 87 100
p = 0,0410
Table 3.4. Changing CEA levels before and after treatment in patients having
CEA > 5,0ng/ml before treatment
Changing CEA levels before and after treatment
(ng/ml)
n %
Increased 3 8,6
Decreased < 5 14 40,0
Decreased 5 -<10 5 14,3
Decreased 10 -<20 4 11,4
Decreased > 20 9 25,7
Total 35 100
The percent of average CEA levels reduced after treatment: 52,0 ± 27,67%
3.2.5. Assess Response based on the rate of surgery:
Table 3.5. The rate of surgical patients after operation
Type of surgery n %
No surgery 18 20,7
Surgery
Sphincter-preserving 11 12,6
Miles 40 46,0
Hartmann 8 9,2
Ostomies 10 11,5
Total 87 100
Table 3.6. General response after treatment
Response n %
Complete Response 8 9,2
Partial Response 71 81,6
Stable Disease 2 2,3
Progressive Disease 6 6,9
Total 87 100
12
Table 3.7. Multivariate analysis of the correlation between response after
radiochemotherapy with some factors
Some factors β α R R
2
p
Group of age -0,164
0,393 0,537 0,288
0,02
Sex -0,015 0,79
% dose compared with
standard dose
0,053 0,463
Stage pre-treatment 0,207 0,002
Type histopathological 0,078 0,391
CEA pre-treatment 0,106 0,075
3.2.6. Assess Response based on histopathology after surgery:
69 patients underwent surgery, but only 59 patients were resected and 54
patients assessed the tumor regression after radiochemotherapy
Figure 3.3. The tumor regression grade in histopathology after operation
Table 3.8. Multivariate analysis of the correlation between tumor regression
grade after radiochemotherapy with some factors
Some factors β α R R
2
p
Group of age -0,138 2,359 0,503 0,253 0,438
Sex 0,078 0,551
% dose compared with standard
dose
0,077 0,618
Stage pre-treatment -0,283 0,110
Type histopathological 0,146 0,537
CEA pre-treatment -0,065 0,622
13
pT -0,231 0,10
Response after
radiochemotherapy
0,146 0,562
Table 3.9. Follow-up 36 months of treatment
n %
Stability 69 79,3
Recurrence, metastasis 8 9,2
Deaths 10 11,5
Total 87 100
14
3.3. Side effects (toxicities) during and after treatment
3.3.1. Hematological toxicities:
Figure 3.4. Changing Hemoglobin toxicity grade before and after treatment
Figure 3.5. Changing Platelets toxicity grade before and after treatment
Figure 3.6. Changing Leukocytes toxicity grade before and after treatment
Figure 3.7. Changing Neutrophils toxicity grade before and after treatment
3.3.2. Hepatic renal toxicities:
Table 3.10. Hepatic renal toxicities
Grade of
toxicity
Before treatment After treatment
n % n %
Creatinin
0 83 95,4 84 96,6
1 3 3,5 3 3,4
2 1 1,1 0 0
Total 87 100 87 100
p = 0,605
AST
0 82 94,3 77 88,5
1 5 5,7 8 9,2
2 0 0 0 0
3 0 0 2 2,3
Total 87 100 87 100
p = 0,241
3.3.3. Other side effects
Table 3.11. Other events in Gastrointestinal tract
Side effects Grade n %
Nausea
0 67 77,0
1 18 20,7
2 2 2,3
Vomiting
0 69 79,3
1 16 18,4
2 2 2,3
Stomatitis
0 86 98,9
1 1 1,1
Diarrhoea
0 82 94,3
1 4 4,6
2 1 1,1
Total 87 100
Bảng 3.12. Hand foot syndrome
Grade n %
15
No symptom 84 96,6
Grade 1 3 3,4
Grade 2, 3 0 0
Total 87 100
Bảng 3.13. Side effects of radiation therapy on the gastrointestinal tract
Side effects
Grade 1 Grade 2
Grade 3, 4,5
n % n %
Anorectal mucositis 11 12,6 0 0 0
Anorectal ulcer 7 8,0 4 4,6 0
Small intestinal mucositis 15 17,2 0 0 0
Rectal perforation 0 0 0 0 0
Rectal obstruction 0 0 0 0 0
Total 87 patients
Bảng 3.14. Side effects of radiation therapy on genital-urinary tract
Side effects
Grade 1 Grade 2
Grade 3,
4, 5
n % n %
Cystitis noninfective 20 23,0 8 9,2 0
Vaginal inflammation 7/38 female 18,4 0 0 0
Total 87 patients
Bảng 3.15. Side effects of radiation therapy on the skin
Side effects
Grade 1 Grade 2
Grade 3, 4,5
n % n %
Pelvic pain 11 12,6 10 11,5 0
Skin ulceration 7 8,0 4 4,6 0
Total 87 patients
Bảng 3.16. The other undesirable effects
Symptoms Patients with symptoms /87 %
Perineal erythema Inflammation 34/87 39,1
Alopecia grade 1 1/87 1,1
Interrupt treatment 12/87 13,8
16
CHAPTER 4: DISCUSSION
4.2. Response after treatment
4.2.1. Functional response
Patients were asked and self-identified about functional response: 100%
patients had functionally responded including 86.2% patients improved ≥ 50%. It
suggested that the effectiveness of treatments helped the patients to improve on
specific symptoms specially with anxiety and discomfort symptoms such as bloody
diarrhea, tenesmus, abdominal pain, weight loss. This is appropriate with Vo Quoc
Hung (2004): 100% patients improved functional symptoms
Tumor volume compared with rectal circumference decreased after
treatment: specially 2.3% patients with non-palpable tumors. Prior treatment, there
were no patients with tumors less than half the circumference, but after treatment
this percentage increased to 29.9%. The proportion of patients with tumor volume
occupied entire circumference decreased from 52,9% before treatment to 16.1%
after treatment. The difference is significant with p <0.001. It suggested that the
effects of treatment: tumor size reduced after treatment. Study of Vo Quoc Hung
also showed the symptoms improved after treatment and the percentage of group
accounted for 1/4 and 1/2 rectal circumference increased. 41.0% patients had
smaller tumor size ≥ 50%. Assess tumor volume compared with rectal
circumference was important for evaluating the response after treatment. The rate
of patients in stage 3, 4 was 70.1% and 29.9% respectively and equivalent with Vo
Van Xuan (2012): tumor stage T3, T4 was 67.9% and 32.1%. In response after
treatment: The number of patients in stage 3 and 4 were down-stage for both stages
comparing with before treatment: 29% of patients in stage 4 has dropped to 11.5%
after treatment, 46.0% (40/87) patients were down-stage for both stages 3 and 4.
The rate of tumor stage 4 reduced into stage 3 was 61.5%, higher than Vo Quoc
Hung (2004): 51.8%. It may be the reason that we combined chemoradiation
therapy for advanced rectal cancer patients but Vo Quoc Hung have used radiation
therapy alone. Soumarova R et al (2010): They acquired data of 78 patients from 1
January 2005 to 31 December 2007 with a locally advanced rectal cancer. All
patients were indicated for the neoadjuvant concomitant chemoradiotherapy due to
locally advanced tumor (T3 or T4) or lymph nodes involvement suspicion (N+).
Both radiotherapy (to pelvic region) and chemotherapy (capecitabine) were
administered. Downstaging was achieved in 69% of patients.
4.2.2. Assessing Response based on pelvic MRI 1.5 Tesla:
Due to the patient’ economic conditions and some patients had previously
implanted metallic part in the body, only 54/87 (62.1%) patients received pelvic
MRI before and after treatment. The downstage was 44.4% after treatment.
Especially 13.0% patients reduced to stage 1 or undetected abnormalities on MRI.
17
By comparing the tumors and lymph nodes on 1.5 Tesla MRI we can assess
objectively the response rate after treatment.
35/54 (64.8%) patients had block-tumor on MRI. 94.3% patients had
reducted tumor volume after treatment, in which 40.0% patients decreased tumor
volume over 10,000mm
3
. If we assessed only the largest lesion diameter of the
tumor before and after treatment, the changing was not too big. But while
compared the tumor volume we assessed more exact about the response rate.
However, we can not calculate the tumor volume on all patients, especially in the
case of the linear form tumors.
Nougaret S Fau – Fujii et al (2012) studied sixteen patients treated by
chemotherapy, radiochemotherapy and surgery. Authors used MRI for assessing
the tumor volume before and after treatment. The mean of tumor volumes was 132
cm(3) ± 166 before and 56 cm(3) ± 71 after chemoradiation. Authors also found
that tumor volumes after treatment were proportionally decreased with the reducing
degree of tumor stage.
4.2.3. Assess Response by comparing the changement of CEA levels
CEA is the main marker of colorectal cancer. The researchers testing the
serum CEA showed that 5ng/ml as the limit of upper normal. Before treatment
59.8% patients had CEA levels ≤ 5.0ng/ml, after treatment this percentage rose to
73.6%. Author Vo Quoc Hung studying radiation therapy for rectal cancer patients
also found the effectiveness. CEA levels decreased after treatment: 46.2% patients
have had CEA ≥ 5ng/ml before radiotherapy reduced to 29.5% after treatment. Our
study had the ratio of CEA > 5ng/ml is higher than Vo Quoc Hung but lower than
Tran Bang Thong: 44.7% of his patients with CEA < 5ng/ml, 25.5% of patients
had CEA 5-10ng/ml and 29.8% of patients with CEA > 10ng/ml. Tran Bang Thong
explained that may due to his selection both distant metastasis patients to the
research, so CEA levels were high before treatment.
For patients with high CEA levels before treatment, we can assess
therapeutic response through the changes of CEA levels before and after treatment.
We conducted paired comparison in each patient about CEA levels before and after
treatment in 35 patients, whose pre-treatment CEA levels were >5.0ng/ml and
showed a significant statistic difference with p = 0.001 (95% confidence). 8.6%
(3/35) of patients with increased CEA levels after treatment coincidence with 3
clinical cases of disease progresses. The remain cases had decreased the CEA
levels after treatment (91.4%) in which, 5.7% of patients with CEA levels reduced
over 20ng/ml after treatment.
According to univariate analysis, 3 factors affected the response after treatment:
age, stage and CEA levels before treatment. Patients aged ≥ 50 years old, stage 3,
CEA levels ≤ 5 ng/ml before treatment had higher response rate than patients <50
18
years of age, stage 4, CEA levels> 5ng/ml (with p <0,05). Other factors such as
gender, histological type and degree, response status, but there were not statistically
significant differences. However, when conducted multivariate analysis the result was
only two factors affected on response: age and stage before treatment.
4.2.4. Assess Response based on the rate of surgery:
79.3% patients were undergoing surgery, in which 67.8% patients radical
surgery, 12.6% of patients underwent anal sphincter preservating
surgery. Compared with studies in other countries the rate of surgery is lower. In
Vo Van Xuan’ study (2012) the Miles’ surgery rate was 48.2%, 10.7% Hartmann,
anal sphincter conservation: 23.2%; ostomies: 17.9%. According to the research by
Vo Quoc Hung (2004): the rate of radical surgery 78.5% in which 21.4%
conservation surgery. It was explained by the proportion of surgical patients in this
study were not high (20.7%), many patients had improved the functional symptoms
and the patients were afraid to bring artificial anus. We had to convince our patients
to surgery, but they refused operation, so some other patients had disease
progression, Examing rectal after treatment we recorgnised the tumors fixed and
invaded sacral and adjacent organs, inoperable. So patients were continued to treate
by radiation and chemotherapy.
Table 4.1. Complete response rate in histopathological after preoperative
radiachemotherapy treatment for rectal cancer patients
Research n Complete response rate (%)
Kim JC et al (2005) 95 12
Elwanis M et al (2009) 43 9,3
De Bruin AF et al 60 13
Soumarova R Fau et al (2010)
78 10
Pham Cam Phuong (2013) 87 9,2
90.8% of patients had response after treatment in which 9.2% of patients
achieved complete response (no cancer cells on postoperative histopathology). The
response rate was higher than Vo Van Xuan (2012): complete response rate was
8.9%, partial response was 73.2%, so 82.1% total response. The reason is that we
have combined chemotherapy and radiation therapy but Vo Van Xuan used
radiation therapy alone for locally advanced rectal cancer patients
Compared with other studies in the world the complete response rate of this
study is lower, it may be explained by number of operative patients was low
because of refusing surgery
4.2.5. Assess Response based on histopathology after surgery:
19
In operated patients, 8 cases achieved complete response on histopathology
and 46 patients had partial response. We conducted immunohistochemical for
evaluation some charecteristics on the histopathology. The majority of patients had
a degeneration and fibrously regenerated tissue reaction after radiochemotherapy.
14.8% of patients achieved 100% degeneration after radiochemotherapy;
68.5% patients had tumor regression < 50%. According to univariate regression
analysis, there were 2 factors affected on tumor regression: stage before and after
treatment (p <0.05). Other factors such as age, sex, percentage dose compared with
standard dose, histological type, histological degree of tumor, CEA levels before
treatment and response status were not statistically significant differences with p>
0.05. However in multivariate regression analysis, there was no factors affect on
tumor regression grade.
With 3-year follow-up, the recurrence and metastasis rate was 9.2%. The
mortality rate was 11.5%. This rate is lower than the local authors: Doan Huu Nghi
studied rectal cancer patients treated by preoperative radiotherapy with dose of 35
Gy then surgery and postoperative radiotherapy, the rate of recurrence, metastasis
after 36 months was 26.9%, the mortality rate was 30.8%. Pham Quoc Dat
researching preoperative radiotherapy with 36Gy dose combined with surgery for
45 patients at the K Hospital from 6/2000 to 11/2001 informed the recurrence rate
and metastasis after 5 years was 50%. The author clarified that the success reason
was the higher applied radiation dose (46Gy) and it combined with capecitabine,
after operation patients also continued to treat by chemotherapy, so the rate of
recurrence and metastasis were more improved.
The resuls of this study showed that a preoperative radiotherapy was
effective for advanced rectal cancer patients because it helped to down-stage,
increased the rate of radical and anal sphincter-preserving surgery.
4.3. Assess the side effects (toxicities) befere and after treatment:
4.3.1. Hematological toxicities:
Before treatment, some patients had anemia and low hemoglobin so at that
time they were indicated blood transfusion. 8.0% of patients with hemoglobin <100
g/l but this proportion increased to 12.6% after treatment. This suggested the
treatment process also affected to bone marrow, the anemia was improved after
treatment. Thereford, during and after treatment (preparation for surgery) some
patients were indicated blood transfusion and medication stimulating bone marrow
to make red blood cells.
On the hematopoietic system, thrombocytopenic toxicity was the most
difficult to recovery and clinicians often worry about this toxicity because if
platelet is lower the patients easely have bleeding symptoms including most
20
dangerous cerebral and gastrointestinal hemorrhages. In this study, no patient had
2,3,4 grade of low platelet, only 10.3% patients had a 1 grade of thrombocytopenia,
none of patients had a symptomatic hemorrhage and no patient had a platelet
transfusion.
In addition to hematological toxicity was anemia and thrombocytopenia,
during radiochemotherapy, the clinicians needed to evaluate the number of
leukocytes. If patients had leukopenia they may have a risk of infection and death.
84.0% patients had normal leukocytes and 16.0% patients had a 1,2,3 grade of
lower white blood cell but patients had any infection syndrome. 85.2% of patients
had normal neutrophils, 12.6% patients had a 1 grade of low neutrophil, 1.1% of
patients had a grade 2 low neutrophil, only 1.1% had a grade 3 of neutropenia after
treatment. The patients were closely monitored and indicated drugs which can
stimulate bone marrow to make leukocytes and used prophylactic antibiotic
treatment. 1 patient with a grade 3 of neutropenia and the treatment was broken a
few days. The changes of leukocytes and neutrophils number before and after
treatment were statistically significant with p = 0.039 and 0.044 respectively. This
shows that the hematological toxicity was low, mainly with grade 1, 2. Acceptable
and low toxicity, only one patient had to stop treatment during one week due to
hematological toxicity.
This result is consistent with the Elwanis M et al (2009): the toxicity mainly
were moderate and no patient had to discontinue treatment. Grade 2 of anemia
occurred in 4 patients (9.3%), 2 patients (4.7%) had leucopenia and dermatitis
encountered in 4 patients (9.3%). That was similar to Kim JC (2005): garde 3
toxicities were few (3% of patients with diarrhea, and only 1% of patients with
neutropenia). Author Kim JS et al (2002): no grade 3, 4 of hematologic toxicity.
Slampa P Fau - Kocakova et al (2004): 3% of patients with grade 3 of leucopenia.
4.3.2. Hepatic and renal toxicities:
When using systemic chemotherapy, clinicians should have monitoring on
hepatic and renal toxicity. If the toxicity was severe we needed to stop the
treatment, reduce the dose and use diuretics, hepatic support medicaments.
Before treatment, 4.5% of patients with high creatinine levels, particularly
one patient had a creatinine levels > 170μmol/l before treatment due to ureteral
compressive lesions, but patients recovered after radiochemotherapy. After
treatment the number of patients with increased creatinine grade 1 fell to 3.4%, it
shows the chemotherapy drugs were safe.
In Vietnam, the incidence of B hepatitis is high so when using chemotherapy
some patients may have an acute hepatitis and affect their lives. Therefore, patients
needed to be asked about history of hepatitis, made hepatitis virus tests before
21
treatment in order to prognosis and prepare for treatment. Before treatment 5
patients (5.7%) had increased grade 1 of AST, and it increased 9.2% after
treatment. No patient had increased a grade 2, 4 of AST; 2.3% of patients had a
grade 3 of AST. In general, hematological and hepatic, renal toxicity mainly were
grade 1.2 and can be recovered.
There was a little effect on hepatic and renal functions. The difference of
mean creatinine values before and after treatment was not statistically significant
with p = 0.16. Comparing the average value of AST before and after treatment
there was any statistically significant difference with p = 0.145.
4.3.3. Other side effects:
The combination of chemotherapy and radiotherapy before surgery in order
to improve a effectiveness of treatment for low locally advanced rectal cancer
patients had less adverse effects, high safety and the patient could tolerate.
In this study, the dose of capecitabine was lower than those using in other
regimens (825mg/m
2
dose vs 1250mg/m
2
) so the side effects was acceptable and
not high. The majority of patients had a grade 1 and 2 adverse effects from
chemotherapy, it didn’t affect to patient's life. 23% of patients had nausea, mainly
grade 1,2 in which the grade 1 was 20.7%. 20.7% of patients vomiting grade 1 and
2, in which mainly level 1 (18.4%). 1.1% of patients with grade 1 of alopecia. 4.6%
of patients with level 1 diarrhea and 1.1% of patients with a grade 2 diarrhea.
There were 3 patients with mild hand foot syndrome but the patients do not must to
be stopped the treatment. After treatment this syndrome also gradually decreased
Author Corvo R et al (2003): the study using capecitabine during
radiotherapy (825 mg/m2/day through a bid administration). Severe hand-foot
syndrome occurred in 7-15% of patients, representing the most commonly observed
toxicity. It is noteworthy that severe diarrhea with capecitabine during radiotherapy
was not common. Leukopenia frequently occurred but was mild and reversible.
Research shows that a high probability of pathological complete response (up to
31%) with capecitabine and radiation, with an increased probability of sphincter-
sparing surgical procedures. Soumarova R Fau et al (2010) acquired data of 78
patients from 1 January 2005 to 31 December 2007 with a locally advanced rectal
cancer in study. All patients were indicated for the neoadjuvant concomitant
chemoradiotherapy due to locally advanced tumor (T3 or T4) or lymph nodes
involvement suspicion (N+). Both radiotherapy (to pelvic region) and
chemotherapy (capecitabine) were administered. Rectal tumors were localized
within 12 cm from the anocutaneous verge. All patients completed their treatment
according to the planned regimen and dose Grade 3 toxicity of the concomitant
chemoradiotherapy was present in 3%; grade 2 in 29% of patients, particularly skin
and gastrointestinal form. They demonstrated safety and low toxicity of the
concomitant chemoradiotherapy with capecitabine.
22
Rectum is an organ located in the pelvis, adjacent to the bladder, uterus,
vagina, prostate, small intestine, sacrum, femur and pelvis. So when using radiation
therapy to rectal tumor, other surrounding organs will be affected and cause
discomfort to the patient. Radiative experts worry the dose could affect to the
bladder, intestines, vagina, prostate and femur
Previously in Vietnam only Cobalt 60 radiation machines were used, so no
high-dose radiotherapy (36Gy) but there was so many side effects,. Since 2000 at K
Hospital and from 2007 at Bach Mai Hospital, linear accelerator systems with 3-
dimensional conformal radiation therapy are applied, improving dose at 46Gy and
desired effect can be accepted.
Comparing with the study of authors Vo Quoc Hung, Pham Quoc Dat: the
ratio of cystitis and painful anus, skin ulcers in treated area in this study was lower.
In the Vo Quoc Hung's research (2004), the complications of preoperative
radiotherapy included: hot and perineal pain 83.9%, cystitis 33.9%, 16.9%
digestive disorders, 8.9% ulcers and radiation fibrosis; 7.1% intestinal adhesion.
Pham Quoc Dat noted perineal erythema inflammatory in 100% of cases; cystitis
73.3%, 13.3% gastrointestinal disorders (diarrhea) and 100% of patients with
perineal pain. The difference may be explained that we have used linear accelerator
system with 3D radiation therapy, so surrounding healthy lessions should be
protected.
During chemoradiotherapy, it should be noted both the side effects of
chemotherapy and radiation therapy. The digestive system is often early affected of
the these effects. With a dose radiotherapy of 46Gy in pelvic area, the organs
around such as small intestine, bladder and vagina are affected. 18.4% of female
patients had mild vaginitis, acceptable. 32.2% of patients had cystitis grade 1 and 2,
but only 8 patients (9.2%) with symptoms of urgency, dysuria and should be used
antibiotics.
The most dangerous side effects in abdominal when radiation are bowel
necrosis, intestinal perforation. In this study there are no patient with intestinal
perforation and obstruction during radiotherapy. However, 17.2% of patients with
symptoms of mild intestinal inflammation, no need for drugs, 12.6% of patients
with anorectal mucositis grade 1. 4.6% of patients with anorectal ulcer grade 2 and
8.0% of patients with anal-rectal ulcers level 1. These patients are often
accompanied by skin ulceration of the anal margin after radiation. In some cases we
have to use additional treatment for ulceration caused by radiation to reduce these
undesirable effects.
Despite 39.1% of patients with symptoms erythema inflammation skin on
treated area, but only 12.6% of patients with perineal skin ulceration, causing
perineal pain. For each patient, there are different pain threshold, some patients
have perineal skin ulceration but without analgesic, some cases needed to use
23
analgesics. 13.8% of patients had ulcers and perineal pain, leukopenia, they were
pause capecitabine and radiation therapy until symptoms have reduced (usually 5-7
days).
The side effects of radiation therapy was higher than some authors in the
world. It could be due to the patient's state, the diet and the radiotherapy system of
Vietnam and foreign countries are different. Author Kim JS et al (2002): Grade 3
toxicities were as follows: hand-foot syndrome (7%), fatigue (4%), diarrhea (4%),
and radiation dermatitis (2%).
The results of this research show that the side effects was acceptable, didn’t
affect to the treatment and patient's life.
CONCLUSION
The results of our study on 87 patients with low locally advanced rectal
cancer treated by preoperative capecitabine and radiotherapy at the Center of
Nuclear Medicine and Oncology, Bach Mai Hospital and Department of 4
th
Radiation, K Hospital from 6/2009-12/2012 show:
1. Effective treatment:
Radiation therapy combined capecitabine before surgery was effective for
low locally advanced rectal cancer, improved functional symptoms, down-stage,
increased the rate of radical and anal sphincter preserving surgery:
- 100% patients had functional response
- 46.0% patients with down-stage
- Tumor volume with rectal circumference decreased after treatment. Before
treatment: 52.9% of the patients with entire circumferent tumors dropped to 16.1%.
2.3% of patients with non-palpable tumors after treatment.
- 40.0% patients had the tumor volume fell over 10,000 mm
3
on 1.5 Tesla
MRI
- 40.2% patients with CEA levels > 5ng/ml before treatment in which 91.4%
patients had reduced CEA levels.
- 79.3% patients underwent surgery in which 67.8% patients with radical
surgery, 12.6% patients underwent anal sphincter preserving surgery
- 90.8% patients achieved a response after treatment and 9.2% patients
complete response
- 62.1% (54/87) of patients assessed response rate on postoperative
histopathology in which 31.5% of patients with grade 3,4 of tumor regression
24
- There was a correlation between age, the before treatment stage with the
after treatment response
- 9.2% patients with recurrence and metastasis, 11.5% patients died during
the follow-up of 36 months
2. Side effects:
Radiotherapy combined preoperative capecitabine regimen for low locally
advanced rectal cancer was safe, acceptable, low toxicity:
- The undesirable effects on hematological, hepatic, renal system were
mostly level 1, 2.
- Nausea, vomiting, stomatitis, diarrhea with low rates: 23.0%, 20.7%, 1.1%,
5.7%, respectively. 3.4% of patients with hand foot syndrome grade 1.
- 17.2% of patients with small intestinal inflammation, 12.6% of patients
with anorectal mucositis and 12.6% of patients with anorectal ulceration, mainly
grade 1.
- 39.1% of patients red inflamed skin on treated area, 12.6% skin ulcers;
24.1% of patients with anal pain level 1 and 2. 32.2% of patients with cystitis and
18.4% female patients had vaginitis, mainly grade 1.
- 13.8% of patients interrupted treatment because of the side effects.
RECOMMENDATIONS
1. Preoperative radiochemotherapy (46 Gy + Capecitabine) should be applied
for locally advanced rectal cancer patients because this regime is highly effective,
low toxicity, increase the rate of radical and anal sphincter-preserving surgery
2. It is necessary after treatment to follow up long-term on free progress
survival, relapse, metastasis, over all survival in the group of locally advanced
rectal cancer patients treated by preoperative radiochemotherapy and adjuvant
treatment to make further conclusions about effectiveness