AHA thoracic aortic aneurysm review 2011
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (513.8 KB, 9 trang )
Contemporary Reviews in Cardiovascular Medicine
Medical Therapy of Thoracic Aortic Aneurysms
Are We There Yet?
Peter Danyi, MD; John A. Elefteriades, MD; Ion S. Jovin, MD
A
n aneurysm is defined as a localized dilatation of a
vessel of Ͼ50% of the normal diameter and includes all
layers of the given vessel.1 Aortic aneurysms are divided into
thoracic aortic aneurysms (TAAs), thoracoabdominal aortic
aneurysms (a thoracic aneurysm extending into the abdomen), and abdominal aortic aneurysms (AAAs). Abdominal
aortic aneurysms are reportedly more common than TAAs.
Demographic studies have suggested that among people Ն65
years of age, the prevalence of AAA is Ϸ2.5%.2 Occurring at
a rate of 4.5 to 5.9 per 100 000 person-years, TAAs are less
common.3 Aortic aneurysms (TAA and AAA together) remain the 13th leading cause of mortality in Western countries4 and are probably responsible for 15 000 to 30 000
deaths per year in the United States.5 TAAs are classified into
4 general anatomic categories: ascending aortic aneurysms
(60%), aortic arch aneurysms (10%), descending aortic aneurysms (40%), and thoracoabdominal aneurysms (10%). It is
important to understand the development, pathogenesis, and
clinical course of aortic aneurysms and to develop strategies
that reduce its occurrence, progression, and mortality. This
review summarizes our present understanding of the available
medical therapies for aortic aneurysms and attempts to
determine whether medical therapy for TAA is currently a
viable option. We focus on TAAs whenever possible; however, it should be mentioned that the available literature for
TAA is limited, and most of the preclinical data are obtained
from AAA animal models. Therefore, we use AAA data with
the caveat that it is unclear that extrapolating from AAA data
leads to correct conclusions regarding TAA. There is significant heterogeneity in the aorta and aortic aneurysms in terms
of their epidemiology, structure, mechanics, and biochemical
systems.6 Although animal models of TAAs have been
described7,8 and studied intensively, it is unclear how relevant
they are to the basic and clinical pathology in humans
because they involve either a genetic defect that has not been
described in humans or the surgical creation of thoracic
aneurysms, respectively.
Origin
Aortic aneurysm is an area of medial degeneration of a focal
portion of the aorta that may or may not be accompanied by
inflammation. Extensive extracellular matrix degradation
leads to localized weakening and dilatation of the aortic wall.
In most cases, destruction of the elastic tissue of the media is
found on histology. Several potential mechanisms have been
proposed that lead to the final pathway of tunica media
destruction.
Etiologic factors include genetic disease or mutations such
as Marfan syndrome in which mutations in the gene encoding
fibrillin-1 (FBN1) have been described.9 More than 800
FBN1 mutations that are associated with Marfan syndrome
have been identified. Most mutations occur within repeated
epidermal growth factor–like domains and lead to enhanced
proteolytic degradation and malfunction of fibrillin-1. Marfan
syndrome affects about 1 in 5000 humans. Aortic dissections
and aneurysms have also been reported in people with other
FBN1 sequence variations without exhibiting other Marfan
properties. Other genetic diseases include Ehlers-Danlos
syndrome, familial aortic dissection, and Loeys-Dietz syndrome. Ehlers-Danlos syndrome can be classified into 11
types and results in skin hyperelasticiy. Type IV EhlersDanlos patients are at greater risk of aortic rupture owing to
a defective synthesis of type III collagen; normal aorta is rich
in type III collagen. The prevalence of Ehlers-Danlos syndrome is also Ϸ1 in 5000. Familial aortic dissection results in
aneurysm and dissection of the aorta at a young age.10
Loeys-Dietz syndrome was recently identified in patients
with mutations in the transforming growth factor- receptors
1 and 2. This disease is phenotypically similar to Marfan
syndrome, and patients also develop TAAs and dissections at
an early age.11 The common congenital anomaly of bicuspid
aortic valve, which affects 2% of the population, has been
associated with TAA. From family studies, it is estimated that
Ϸ20% of TAAs are due to genetic diseases. The common
method of inheritance seems to be autosomal dominant.12 In
AAAs, the genetic predisposition is reported to be between
12% and 19%.13
Among other risk factors, smoking has the strongest
association with both TAA and AAA, with a relative risk of
5 for the presence of AAA.14 Current smoking by itself is
estimated to be responsible for 0.4-mm/y additional growth
rate of aortic aneurysms.15 Dyslipidemia and hypertension are
less powerful risk factors, considered to be associated mainly
with the occurrence of AAA, although newer data suggest
that hypertension may actually be more closely associated
with TAA,16 and is certainly a risk factor for dissection. Men
From Virginia Commonwealth University (P.D., I.S.J.) and McGuire VAMC (P.D., I.S.J.), Richmond, VA, and Yale University, New Haven, CT
(J.A.E., I.S.J.).
Correspondence to Ion S. Jovin, MD, 1201 Broad Rock Blvd 111J, Richmond, VA 23249. E-mail
(Circulation. 2011;124:1469-1476.)
© 2011 American Heart Association, Inc.
Circulation is available at
DOI: 10.1161/CIRCULATIONAHA.110.006486
Downloaded from />by guest on September 16, 2015
1469
1470
Circulation
September 27, 2011
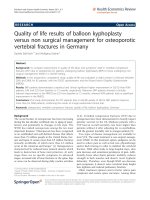
Figure. Molecular mechanisms of aneurysm
formation and the effects of different medications. Angiotensin promotes aneurysm formation through angiotensin 1 (AT1) receptors.
Increased angiotensin II causes an increase in
reactive oxygen species (ROS) through the
NADH/NADPH system, which in turn increases
cyclophilin A and matrix metalloproteinase
(MMP) levels. This promotes inflammatory reaction and subsequent medial degeneration,
leading to aneurysm formation. Fibrillin gene
mutations cause enhanced transforming growth
factor (TGF)- signaling. This results in cellular
proliferation and matrix degradation probably
through signaling via the psmad2 system. Angiotensin receptor blockers (ARBs) are thought
to inhibit the above pathways via inhibition of
the AT1 receptors. Angiotensin-converting
enzyme inhibitors (ACEIs) block angiotensin II.
Statins block the NADH/NADPH system; tetracyclines and macrolides reduce MMP activity.
-Blockers reduce shear stress on the vessel.
are more often affected than women. Advanced age, hypertension, chronic obstructive lung disease, and coronary artery
disease are also associated risk factors for both TAA and
AAA,2 although it should be noted that not all studies identify
hypertension and coronary artery disease as risk factors for
AAA. They are not only risk factors for the presence of
aneurysm, but also dominant determinants of aneurysm
growth and rupture.17 Uncommon causes include bacterial
endocarditis or infection of a laminal clot (from Staphylococcus aureus and S. epidermidis, Salmonella, and Streptococcus
species), as well as syphilis, Takayasu arteritis, and giant-cell
arteritis (temporal arteritis). Dissection is also considered a
risk factor for thoracic aneurysm, and patients who undergo
thoracic dissection repair are at some risk of forming aneurysms in other segments of their thoracic aorta.18,19 However,
it is unclear whether dissection is a true risk factor or
dissection was the first manifestation of the aneurysmal
disease. Diabetes mellitus may be associated more closely
with AAA than with TAA,16 although several other studies
actually suggest an inverse association between diabetes and
AAA (ie, patients with diabetes mellitus are less likely to
develop AAA).2
Pathophysiology
All of the above causes and risk factors exert their effects
through localized inflammatory changes, culminating in degradation of extracellular matrix and apoptosis of vascular
smooth muscle cells, which used to be described as cystic
medial necrosis but is now more accurately called medial
degeneration of the aortic wall. Medial degeneration is a
nonspecific degenerative condition that provides the anatomic background for dissection.20 The precise pathogenesis
that leads to these changes is not fully understood. One
mechanism that has been proposed is the development of
reactive oxygen species that activate matrix metalloproteinases (MMPs), thereby causing an imbalance between MMPs
and their inhibitors (tissue inhibitors of metalloproteinases).
Found to be important in the pathogenesis of both TAAs and
AAAs, MMPs are a family of zinc endopeptidases that are
responsible for the degradation of the extracellular matrix in
aortic aneurysms.21 Matrix metalloproteinase-2 is produced
in mesenchymal cells; MMP-9 is produced in macrophages.
These are required elements of aneurysm formation.22
Ejiri et al23 demonstrated the role of NADH/NADPH
oxidase in the development of reactive oxygen species and its
effect in the development of TAA. Angiotensin II has also
been implicated in the development of aortic aneurysms
through its NADH/NADPH activation in vascular smooth
muscle cells.24 Transforming growth factor- has been seen
in elevated levels in certain aneurysmal segments, notably in
Marfan syndrome and other inherited diseases.25 Transforming growth factor- has been associated with thickening of
the aortic wall and the fragmentation and disarray of elastic
fibers.25 In a recent study, Moran et al26 demonstrated the role
of osteoprotegerin in the growth of AAAs. Osteoprotegerin is
a member of the tumor necrosis factor receptor family.
Osteoprotegerin plays a role in vascular disease; its serum
level increases in atherosclerosis, and it is associated with
AAA size.27 Recombinant human osteoprotegerin inhibits
vascular smooth muscle cell proliferation and induces apoptosis.26 Satoh et al28 recently identified cyclophilin A as a
key factor in the development of aortic aneurysms via the
inflammatory response to angiotensin II through reactive
oxygen species. It is possible that all of the above-described
pathways are part of a common inflammatory cascade.29
Finally, the mitogen-activated protein kinase/extracellular
signal-regulated kinase cascade has also been implicated in
aneurysm formation. This signal transduction pathway is very
complex, involves a large number of proteins, and serves to
couple intracellular responses to the binding of growth factor
to cell surfaces. Inhibition of this pathway with statin and
extracellular signal-regulated kinase inhibitors has been
shown to reduce AAA formation in experimental models.30
An overview of potential cellular pathways leading to aortic
aneurysm is depicted in the Figure.
Biomarkers and Genetic Markers
Thoracic aortic aneurysm is a virulent, potentially lethal, but
predominantly silent disease. There are significant challenges
in diagnosing and following the growth of aneurysms.31
Downloaded from by guest on September 16, 2015
Danyi et al
Recent understanding of the pathophysiology of aneurysmal
disease led to the search for potential biomarkers for both the
presence and growth of aneurysms. Indicators of ongoing
thrombosis, inflammatory markers, MMPs, markers of collagen turnover, genetic markers, and other potential markers
have been evaluated,32 but the promise of biomarkers has not
been realized.33
As has been noted, a significant portion of TAA disease is
genetic (Marfan syndrome, Loeys-Dietz syndrome, familial
TAA and dissection syndrome, Ehlers-Danlos syndrome type
IV). Mutations have been described in the FBN1 gene,
transforming growth factor- receptor gene type 1 and 2
(TGFBR 1 and 2), and smooth muscle–specific isoforms of
-myosin and ␣-actin genes (MYH11 and ACTA2). Recent
data have improved our understanding of the role of genetic
factors in altered smooth muscle cell contraction and the
pathogenesis of TAAs.34 The genetic predisposition for AAA
is multifactorial, and recent genome-wide association studies
have shown associations between AAA and loci on chromosomes 9p21.335 and 9q33.36 Genetic testing is available for
family members of TAA patients, but routine screening is not
yet advisable because of cost and practicality; hundreds of
mutations in these genes have been associated with TAA, and
the usefulness of genetic testing has not been proven.37
Clinical Course
The major cause of mortality from aortic aneurysm is
dissection and rupture. Most aneurysms are clinically silent.
If symptoms are present, they can include heart failure, chest
pain, myocardial ischemia, back pain, and flank pain. Compression of branch vessels can produce ischemia in the
corresponding territories. According to the law of Laplace, as
the size of the aneurysm increases, the wall tension rises, even
though the relationship is potentially altered by the fact that there
often is compensatory aortic thickening through remodeling,
which may reduce the tension. There is a rising incidence of
dissection and rupture with expanding aneurysm size.38 Studies
show that the overall incidence of aortic dissection in the general
population is 2.9 to 3.5 per 100 000 person-years.39 The growth
rate of aneurysms is estimated to be between 0.1 and 0.4 cm/y,40
making accurate measurements of change and clinical trials
challenging. The rates of dissection and rupture of TAAs are
also dependent on aneurysm site (ascending or descending
aorta). In the ascending aorta, we see a steep increase in
complication rates once the aneurysm exceeds 6 cm in
diameter. Above that diameter, the rate of aortic dissection
and rupture increases to Ͼ30% a year. In descending aortic
aneurysms, this happens when the diameter reaches 7 cm.41
The 5-year survival from untreated TAAs has been reported
to be between 19.2%42 and 64%,3 whereas 8-year survival in
AAA has been reported to be 75% to 80%.40
Therapy
The recommended therapy for aortic aneurysms is dependent
on aneurysm-specific factors (size, location, rate of growth,
origin) and patient-specific factors (risk factors, comorbidities, presence of complications from the aneurysm). Available therapies are open and endovascular surgeries, medical
therapies, and lifestyle modification.
Medical Therapy of TAA
1471
Open and Endovascular Surgical Therapy
Historically, surgical repair of aortic aneurysms was suggested after it was noted that most aneurysms rupture before
they reach 10-cm diameter.43 Current recommendations44 are
to repair an ascending TAA at 5.5-cm diameter (5.0 cm in
case of Marfan patients) and a descending TAA at 6.0 cm if
repaired with open surgical technique and 5.5 cm if repaired
with endovascular technique (5.5 cm for Marfan patients) or
if the rate of growth is Ͼ1 cm/y. Other indications are
concurrent aortic insufficiency and surgical emergencies
from aneurysm complications.44,45 These recommendations
are based on the inherent risk of surgery being lower than the
annual risk of aortic rupture for sizes larger than the above
size criteria. Open surgical repair has a surgical mortality rate
of 5% to 10% for elective TAA repair and up to twice as high
for nonelective operations,46 with lowest values for ascending
aneurysm repair and highest values for thoracoabdominal
aneurysm repair. Recently, low-risk thoracic aortic surgery
has been reported at specialized aortic centers.47 The risk of
spinal cord ischemia causing paraplegia is 5% to 10%48 with
open TAA repair in descending operations only.
Covered stent grafts have been available in the United
States for endovascular aneurysm repair since 2005. Current
recommendations are for infrarenal AAA repair and descending TAA repair in aneurysms that are without abdominal
extension.49 The perioperative mortality and 30-day mortality
have been reported to be lower than for open repair,50 but the
durability of benefit has been questioned. A recent systematic
review of open versus endovascular TAA repair seems to
confirm the lower risk of death with endovascular repair, but
those authors cautioned that the quality of the studies was not
good.51 A review of survival data on Ͼ11 000 Medicare
patients with TAAs showed a reduced 30-day mortality but
similar 5-year mortality between open and endovascular
repair.52 Recently, hybrid procedural approaches have been
reported in which open and endovascular procedures are
used.53 From randomized trial data, there is no evidence for a
midterm survival benefit when comparing medical and endovascular repair for either AAA (Endovascular Aneurysm
Repair-2 [EVAR-2]) or TAAs (Investigation of Stent Grafts
in Aortic Dissection [INSTEAD]) or when comparing open
and endovascular repair for AAAs (Dutch Randomized Endovascular Aneurysm Management [DREAM]).31 The
EVAR-2 and DREAM trials were done in patients with AAA
and compared conservative therapy with endovascular repair
and open repair with endovascular repair, respectively. The
INSTEAD trial,54 which compared medical therapy with
endovascular therapy in patients with aortic type B dissection,
showed no benefit of endovascular therapy over medical
therapy but was underpowered for the chosen end points and
was criticized because of the long period of time allowed
from the time of dissection to enrollment and the high
crossover rate.
The more recently introduced fenestrated endografts also
enable an endovascular approach to thoracoabdominal aortic
aneurysms and complex aneurysms. However, there is little
evidence of the long-term durability and efficacy of this
approach.
Downloaded from by guest on September 16, 2015
1472
Circulation
September 27, 2011
Medical Therapy
Principles and Goals of Medical Therapy
The goals of medical therapy have traditionally been to
reduce shear stress on the aneurysmal segment of the aorta by
reducing blood pressure and contractility (dP/dt). Although
there is little evidence that cardiovascular risk factor reduction influences outcome in aortic aneurysm to a great degree,
it has traditionally been recommended that cardiovascular
risk factor reduction takes place. More recently, numerous
reports have been published of plausible therapies that aim to
affect the underlying pathophysiological changes in aortic
aneurysms, thus modifying the disease process as opposed to
only trying to delay its complications.
Medical Therapy in Acute Aortic Dissection
In acute aortic dissection, appropriate and immediate therapy
is essential with the aim of stabilizing the patient and
improving the clinical outlook. The main goals of therapy are
blood pressure control, decrease of shear stress, optimization
of anticoagulation, volume management, and pain control. A
detailed discussion is beyond the scope of this article but can
be found in excellent published reviews.55,56
Medical Therapy of Chronic Aortic Aneurysm
-Blockers
-Blockers may be beneficial for reducing the rate of aortic
dilatation. This is thought to be due to the effect of -blockers
in reducing left ventricular dP/dt and reducing shear stress. In
addition, -blockers reduce dP/dt in the aorta and might be
beneficial via this mechanism and the resultant effect on
shear stress in the aorta. Several animal studies and other
retrospective clinical studies have also indicated a significant
inhibitory effect of -blockers on aneurysm growth rate.57,58
In a small study of 70 patients with Marfan syndrome,
propranolol-treated patients had a 73% lower rate of aortic
dilatation and lower mortality than placebo-treated patients.59
However, later prospective randomized trials of -blockers in
patients with AAA failed to show a significant effect,60
although there was a trend favoring propranolol.61 These
trials found a low compliance rate with propranolol (a 42%
discontinuation rate in 1 trial) and a significant negative
effect of propranolol on quality of life. At this time, no studies
of -blockers in patients with thoracic aortic disease (other
than Marfan patients62) have been published.
Tetracyclines/Macrolides
Doxycycline is a nonspecific MMP inhibitor.63 This antibiotic has been used in conditions with MMP overexpression
(eg, periodontal disease, rheumatoid arthritis).64 In animal
models, doxycycline slowed elastin degradation and aneurysm development.65 In a small series of human subjects,
doxycycline decreased MMP-9 levels66 and slowed the rate of
progression of AAA in humans.67 The macrolide roxithromycin has also been shown to inhibit the rate of expansion of
AAA in humans, possibly through a similar mechanism.68
Statins
Statin treatment is one of the cornerstone therapies in cardiovascular diseases. Statins reduce the progression of atherosclerosis and improve clinical outcomes. In addition to their
lipoprotein-reducing properties, statins have a number of
effects called pleiotropic effects. For instance, they reduce
oxidative stress by blocking the effects of reactive oxygen
species on aneurysms. This effect is independent of their
lipid-lowering properties. Statins achieve these results
through suppressing the NADH/NADPH oxidase system.23
These effects have been shown in both AAA and TAA
specimens. Aneurysm expansion rate has also been shown to
be reduced in AAA patients on statins in observational
studies,69 but the largest study to date failed to show an
association between statin prescription and AAA growth
rate.70 At this time, no studies of statins in patients with
thoracic aortic disease have been published.
Angiotensin-Converting Enzyme Inhibitors/Angiotensin
Receptor Blockers
Angiotensin II has been shown to have a number of biological
effects on the cardiovascular system. It promotes vascular
hypertrophy, cell proliferation, production of extracellular
matrix, and activation of macrophages, and it activates
NADH/NADPH oxidase of vascular smooth muscle cells.
Angiotensin-converting enzyme inhibitors (ACEIs) have
been shown to both stimulate and inhibit MMPs and the
degradation of extracellular matrix in aortic aneurysms.71
Losartan, an angiotensin I receptor blocker (ARB), seems to
exert its beneficial effect through blocking transforming
growth factor-, thereby reducing matrix degradation in a
Marfan syndrome mouse model.25 In Marfan and apolipoprotein E– deficient mice (in which angiotensin II is infused to
induce aneurysm), ARB (losartan) prevents aneurysm formation and ACEIs do not.25 However, in other animal models of
aneurysm (eg, elastase, -aminopropionitrile monofumarate
models), ACEIs prevent aortic dissection and ARB does
not.72 In 1 small human study, ARB has been shown to slow
the rate of progression of TAA in Marfan syndrome.73
However, Hackam et al74 found in their case-control study
that ACEIs were protective but ARBs were not protective
against AAA rupture, but in that study there was no doseresponse effect for ACEIs and little adjustment for potential
confounders. A recent report of an observational prospective
study of AAA patients showed an increased growth rate of
AAA diameter from 2.77 to 3.33 mm/y in patients on
ACEIs.75 In a recent randomized trial, perindopril was shown
to reduce the growth rate of thoracic aortic aneurysms in
patients with Marfan syndrome.76 The ongoing Study of the
Efficacy of Losartan on Aortic Dilatation in Patients With
Marfan Syndrome (MARFANSARTAN) seeks to address the
efficacy of losartan in Marfan syndrome.77 It appears that the
discrepant results of ARB and ACEI efficacy in retarding
aneurysm growth rate might stem from the differences among
models and point toward multiple different biological pathways of aortic aneurysm development. An overview of
studies reporting results of medical therapy of aortic aneurysm can be found in the Table.
Other Agents
New agents in animal studies that attempted to delay AAA
development have targeted oxidative stress, proteolysis, and
inflammation.78 The clinical efficacy of these approaches in
TAA has yet to be tested. Transforming growth factor-–
Downloaded from by guest on September 16, 2015
Danyi et al
Table.
Medical Therapy of TAA
1473
Clinical Studies of Medical Therapy for Aortic Aneurysms
Authors
Study Design
Intervention
Patients, n
Findings
Marfan syndrome; randomized, prospective
study; Ϸ10-y mean follow-up
Propranolol
32 Treated, 38
control subjects
Propranolol caused significantly reduced
aortic root dilatation
Infrarenal AAA; observational, prospective
study; 43-mo mean follow-up
-blocker
38 Treated, 83
control subjects
Patients with large aneurysms on
-blockers had significantly lower AAA
expansion rate
AAA; observational, retrospective study;
34-mo mean follow-up
-blocker
12 on -blocker, 15
not on -blocker
Patients on -blocker had significantly
lower AAA expansion rate
AAA; prospective, randomized, double-blind
study; 2.5-y mean follow-up
Propranolol
276 on propranolol,
272 on placebo
Propranolol did not significantly affect
small AAA growth; high discontinuation
rate of propranolol
Lindholt et al60
AAA; randomized, controlled study; 2-y
follow-up
Propranolol
54 Asymptomatic
patients
Increased mortality in propranolol group;
only 22% could be treated
Baxter et al66
AAA; prospective, observational study;
6-mo phase II study
Doxycycline
36 Patients
Doxycycline was safe and caused
MMP-9 level decrease
Mosorin et al67
AAA; randomized, placebo controlled,
double-blind study; 18-mo follow-up
Doxycycline
17 on doxycycline,
15 on placebo
Aneurysm expansion rate was
significantly lower in the doxycycline
group
Vammen et al68
AAA; randomized, double-blind study;
1.5-y mean follow-up
Roxithromycin
43 on roxithromycin,
49 on placebo
4 wk of therapy reduced AAA expansion
rate
Sweeting et al75
AAA; prospective, observational study;
1.9-y mean follow-up
ACEI
169 on ACEI, 1532
not on ACEI
Patients on ACEI had a faster AAA
growth rate than patients not on ACEI
Ferguson et al70
AAA; observational, prospective study; 5-y
median follow-up
Statins
394 on statins, 258
not on statins
Statins were not associated with
reduced AAA growth rate
Marfan syndrome; open-label phase III
study
Losartan, nebivolol
291 patients
Ongoing
Shores et al59
Gadowski et al57
Leach et al58
Propranolol Aneurysm
Trial Investigators61
Gambarin62
AAA indicates abdominal aortic aneurysm; MMP, matrix metalloproteinase; and ACEI, angiotensin-converting enzyme inhibitor.
neutralizing antibodies have been used in animal research and
have shown efficacy in delaying or avoiding the development
of TAA in Marfan syndrome.25 Transforming growth factor antagonism therefore might represent a strategy for at least
some forms of aortic aneurysm. Unfortunately, transforming
growth factor-–neutralizing antibody treatment in humans is
not yet practical. In another study, a c-Jun-N-terminal kinase
inhibitor was used to induce regression of AAA in mice.79
Glucocorticoid, leukocyte-depleting antibody (anti-CD 18),
and indomethacine also have been used,80 and early studies
with chymase inhibitors81 and aspirin82 have also shown
promising results. Lifestyle modifications such as smoking
cessation are also very important. Tobacco use is associated
with a marked increase in general morbidity and mortality
and with a 5-fold relative risk increase for the presence of
AAA.83 Pregnancy is not recommended in patients with
Marfan syndrome, especially if the aortic root is Ͼ4 cm.
Conclusions
Aortic aneurysm is still an incompletely known entity that
affects a significant proportion of the population. Multiple
new pathophysiological pathways have been proposed recently; however, the exact mechanisms that can induce
aneurysm formation remain unclear. Surgical repair has
relatively high risk because of the usually complex nature of
the procedure; therefore, surgical therapy is generally reserved until the risk of rupture exceeds that of the surgery.
Recent series have documented substantially increased safety
of thoracic surgery, approaching the safety of traditional
cardiac procedures such as coronary artery bypass graft
surgery and valve replacement. Endovascular repair is a new
possibility that confers less early risk to carefully selected
patients, but midterm results call into question the durability
of endovascular repairs of degenerative aneurysms.
To improve patient safety and outcome, it is imperative to
find treatments that delay or even stop the progression of
aneurysm disease. The ideal treatment would of course be one
that reverses aneurysm formation. Multiple medications have
been tried that are known to act on 1 or more of the proposed
pathophysiological pathways of aortic aneurysm development. Only 2 randomized prospective trials have been carried
out so far, both in patients with Marfan syndrome. Both trials
were relatively small, and only 1 study had clinical end
points. Some treatment options (eg, ACEI, ARB, -blockers)
have shown conflicting results, most likely because of the
multiple causes of aneurysm formation. However, as our
understanding of the disease improves, it is conceivable that
we will have better medical therapies to slow the progression
of thoracic aortic disease. To do so, we must be willing to
randomize patients in clinical trials, and we must also
consider relevant clinical end points rather than focusing
solely on aneurysm expansion. Recently, the heterogeneity of
the aorta itself has been raised as a plausible reason for the
difference in aneurysm pathology and clinical course.6 Although it seems reasonable to treat patients with aneurysms
the same way that any other patients are treated in terms of
cardiovascular risk factors and prevention, the starting of
medications solely to prevent aortic aneurysm expansion is
Downloaded from by guest on September 16, 2015
1474
Circulation
September 27, 2011
endorsed by the most recent guidelines44 as a reasonable
option, even though an argument can be made that we should
wait until we have a more thorough understanding of the
etiologic diversity of aneurysm formation and of the risks and
benefits of each treatment.31
Disclosures
None.
References
1. Johnston KW, Rutherford RB, Tilson MD, Shah DM, Hollier L, Stanley
JC. Suggested standards for reporting on arterial aneurysms: Subcommittee on Reporting Standards for Arterial Aneurysms, Ad Hoc Committee on Reporting Standards, Society for Vascular Surgery and North
American Chapter, International Society for Cardiovascular Surgery.
J Vasc Surg. 1991;13:452– 458.
2. Lederle FA, Johnson GR, Wilson SE, Chute EP, Littooy FN, Bandyk D,
Krupski WC, Barone GW, Acher CW, Ballard DJ. Prevalence and associations of abdominal aortic aneurysm detected through screening: Aneurysm Detection and Management (ADAM) Veterans Affairs Cooperative Study Group. Ann Intern Med. 1997;126:441– 449.
3. Coady MA, Rizzo JA, Goldstein LJ, Elefteriades JA. Natural history,
pathogenesis, and etiology of thoracic aortic aneurysms and dissections.
Cardiol Clin. 1999;17:615– 635; vii.
4. Isselbacher EM. Thoracic and abdominal aortic aneurysms. Circulation.
2005;111:816 – 828.
5. Kent KC, Zwolak RM, Jaff MR, Hollenbeck ST, Thompson RW,
Schermerhorn ML, Sicard GA, Riles TS, Cronenwett JL. Screening for
abdominal aortic aneurysm: a consensus statement. J Vasc Surg. 2004;
39:267–269.
6. Ruddy JM, Jones JA, Spinale FG, Ikonomidis JS. Regional heterogeneity
within the aorta: relevance to aneurysm disease. J Thorac Cardiovasc
Surg. 2008;136:1123–1130.
7. Andrews EJ, White WJ, Bullock LP. Spontaneous aortic aneurysms in
blotchy mice. Am J Pathol. 1975;78:199 –210.
8. Ikonomidis JS, Gibson WC, Gardner J, Sweterlitsch S, Thompson RP,
Mukherjee R, Spinale FG. A murine model of thoracic aortic aneurysms.
J Surg Res. 2003;115:157–163.
9. Biery NJ, Eldadah ZA, Moore CS, Stetten G, Spencer F, Dietz HC.
Revised genomic organization of FBN1 and significance for regulated
gene expression. Genomics. 1999;56:70 –77.
10. Nicod P, Bloor C, Godfrey M, Hollister D, Pyeritz RE, Dittrich H, Polikar
R, Peterson KL. Familial aortic dissecting aneurysm. J Am Coll Cardiol.
1989;13:811– 819.
11. Loeys BL, Schwarze U, Holm T, Callewaert BL, Thomas GH, Pannu H,
De Backer JF, Oswald GL, Symoens S, Manouvrier S, Roberts AE,
Faravelli F, Greco MA, Pyeritz RE, Milewicz DM, Coucke PJ, Cameron
DE, Braverman AC, Byers PH, De Paepe AM, Dietz HC. Aneurysm
syndromes caused by mutations in the TGF-beta receptor. N Engl J Med.
2006;355:788 –798.
12. Albornoz G, Coady MA, Roberts M, Davies RR, Tranquilli M, Rizzo JA,
Elefteriades JA. Familial thoracic aortic aneurysms and dissections:
incidence, modes of inheritance, and phenotypic patterns. Ann Thorac
Surg. 2006;82:1400 –1405.
13. Verloes A, Sakalihasan N, Koulischer L, Limet R. Aneurysms of the
abdominal aorta: familial and genetic aspects in three hundred thirteen
pedigrees. J Vasc Surg. 1995;21:646 – 655.
14. Boll AP, Verbeek AL, van de Lisdonk EH, van der Vliet JA. High
prevalence of abdominal aortic aneurysm in a primary care screening
programme. Br J Surg. 1998;85:1090 –1094.
15. Brady AR, Thompson SG, Fowkes FG, Greenhalgh RM, Powell JT.
Abdominal aortic aneurysm expansion: risk factors and time intervals for
surveillance. Circulation. 2004;110:16 –21.
16. Ito S, Akutsu K, Tamori Y, Sakamoto S, Yoshimuta T, Hashimoto H,
Takeshita S. Differences in atherosclerotic profiles between patients with
thoracic and abdominal aortic aneurysms. Am J Cardiol. 2008;101:
696 – 699.
17. Ramanath VS, Oh JK, Sundt TM 3rd, Eagle KA. Acute aortic syndromes
and thoracic aortic aneurysm. Mayo Clin Proc. 2009;84:465– 481.
18. Heinemann M, Laas J, Karck M, Borst HG. Thoracic aortic aneurysms
after acute type A aortic dissection: necessity for follow-up. Ann Thorac
Surg. 1990;49:580 –584.
19. Yu HY, Chen YS, Huang SC, Wang SS, Lin FY. Late outcome of patients
with aortic dissection: study of a national database. Eur J Cardiothorac
Surg. 2004;25:683– 690.
20. Elefteriades JA. Thoracic aortic aneurysm: reading the enemy’s
playbook. Yale J Biol Med. 2008;81:175–186.
21. Palombo D, Maione M, Cifiello BI, Udini M, Maggio D, Lupo M. Matrix
metalloproteinases: their role in degenerative chronic diseases of
abdominal aorta. J Cardiovasc Surg (Torino). 1999;40:257–260.
22. Longo GM, Xiong W, Greiner TC, Zhao Y, Fiotti N, Baxter BT. Matrix
metalloproteinases 2 and 9 work in concert to produce aortic aneurysms.
J Clin Invest. 2002;110:625– 632.
23. Ejiri J, Inoue N, Tsukube T, Munezane T, Hino Y, Kobayashi S, Hirata
K, Kawashima S, Imajoh-Ohmi S, Hayashi Y, Yokozaki H, Okita Y,
Yokoyama M. Oxidative stress in the pathogenesis of thoracic aortic
aneurysm: protective role of statin and angiotensin II type 1 receptor
blocker. Cardiovasc Res. 2003;59:988 –996.
24. Griendling KK, Minieri CA, Ollerenshaw JD, Alexander RW. Angiotensin II stimulates NADH and NADPH oxidase activity in cultured vascular
smooth muscle cells. Circ Res. 1994;74:1141–1148.
25. Habashi JP, Judge DP, Holm TM, Cohn RD, Loeys BL, Cooper TK,
Myers L, Klein EC, Liu G, Calvi C, Podowski M, Neptune ER, Halushka
MK, Bedja D, Gabrielson K, Rifkin DB, Carta L, Ramirez F, Huso DL,
Dietz HC. Losartan, an AT1 antagonist, prevents aortic aneurysm in a
mouse model of Marfan syndrome. Science. 2006;312:117–121.
26. Moran CS, McCann M, Karan M, Norman P, Ketheesan N, Golledge J.
Association of osteoprotegerin with human abdominal aortic aneurysm
progression. Circulation. 2005;111:3119 –3125.
27. Golledge J, McCann M, Mangan S, Lam A, Karan M. Osteoprotegerin
and osteopontin are expressed at high concentrations within symptomatic
carotid atherosclerosis. Stroke. 2004;35:1636 –1641.
28. Satoh K, Nigro P, Matoba T, O’Dell MR, Cui Z, Shi X, Mohan A, Yan
C, Abe J, Illig KA, Berk BC. Cyclophilin A enhances vascular oxidative
stress and the development of angiotensin II-induced aortic aneurysms.
Nat Med. 2009;15:649 – 656.
29. Weintraub NL. Understanding abdominal aortic aneurysm. N Engl J Med.
2009;361:1114 –1116.
30. Zhang Y, Naggar JC, Welzig CM, Beasley D, Moulton KS, Park HJ,
Galper JB. Simvastatin inhibits angiotensin II-induced abdominal aortic
aneurysm formation in apolipoprotein E-knockout mice: possible role of
ERK. Arterioscler Thromb Vasc Biol. 2009;29:1764 –1771.
31. Elefteriades JA, Farkas EA. Thoracic aortic aneurysm clinically pertinent
controversies and uncertainties. J Am Coll Cardiol. 2010;55:841– 857.
32. Botta DM Jr. Biomarkers for diagnosis in thoracic aortic disease: PRO.
Cardiol Clin. 28:207–211.
33. Farkas EA. Biomarkers for diagnosis in thoracic aortic disease: CON.
Cardiol Clin. 28:213–220.
34. Milewicz DM, Guo DC, Tran-Fadulu V, Lafont AL, Papke CL, Inamoto
S, Kwartler CS, Pannu H. Genetic basis of thoracic aortic aneurysms and
dissections: focus on smooth muscle cell contractile dysfunction. Annu
Rev Genomics Hum Genet. 2008;9:283–302.
35. Bown MJ, Braund PS, Thompson J, London NJ, Samani NJ, Sayers RD.
Association between the coronary artery disease risk locus on chromosome 9p21.3 and abdominal aortic aneurysm. Circ Cardiovasc Genet.
2008;1:39 – 42.
36. Gretarsdottir S, Baas AF, Thorleifsson G, Holm H, den Heijer M, de
Vries JP, Kranendonk SE, Zeebregts CJ, van Sterkenburg SM,
Geelkerken RH, van Rij AM, Williams MJ, Boll AP, Kostic JP, Jonasdottir A, Jonasdottir A, Walters GB, Masson G, Sulem P, Saemundsdottir
J, Mouy M, Magnusson KP, Tromp G, Elmore JR, Sakalihasan N, Limet
R, Defraigne JO, Ferrell RE, Ronkainen A, Ruigrok YM, Wijmenga C,
Grobbee DE, Shah SH, Granger CB, Quyyumi AA, Vaccarino V, Patel
RS, Zafari AM, Levey AI, Austin H, Girelli D, Pignatti PF, Olivieri O,
Martinelli N, Malerba G, Trabetti E, Becker LC, Becker DM, Reilly MP,
Rader DJ, Mueller T, Dieplinger B, Haltmayer M, Urbonavicius S,
Lindblad B, Gottsater A, Gaetani E, Pola R, Wells P, Rodger M, Forgie
M, Langlois N, Corral J, Vicente V, Fontcuberta J, Espana F, Grarup N,
Jorgensen T, Witte DR, Hansen T, Pedersen O, Aben KK, de Graaf J,
Holewijn S, Folkersen L, Franco-Cereceda A, Eriksson P, Collier DA,
Stefansson H, Steinthorsdottir V, Rafnar T, Valdimarsson EM, Magnadottir HB, Sveinbjornsdottir S, Olafsson I, Magnusson MK, Palmason R,
Haraldsdottir V, Andersen K, Onundarson PT, Thorgeirsson G,
Kiemeney LA, Powell JT, Carey DJ, Kuivaniemi H, Lindholt JS, Jones
GT, Kong A, Blankensteijn JD, Matthiasson SE, Thorsteinsdottir U,
Stefansson K. Genome-wide association study identifies a sequence
Downloaded from by guest on September 16, 2015
Danyi et al
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
variant within the DAB2IP gene conferring susceptibility to abdominal
aortic aneurysm. Nat Genet. 2010;42:692– 697.
Elefteriades JA. Genetic testing in aortic aneurysm disease: CON.
Cardiol Clin. 2010;28:199 –204.
Davies RR, Goldstein LJ, Coady MA, Tittle SL, Rizzo JA, Kopf GS,
Elefteriades JA. Yearly rupture or dissection rates for thoracic aortic
aneurysms: simple prediction based on size. Ann Thorac Surg. 2002;73:
17–27.
Meszaros I, Morocz J, Szlavi J, Schmidt J, Tornoci L, Nagy L, Szep L.
Epidemiology and clinicopathology of aortic dissection. Chest. 2000;117:
1271–1278.
Lederle FA, Wilson SE, Johnson GR, Reinke DB, Littooy FN, Acher
CW, Ballard DJ, Messina LM, Gordon IL, Chute EP, Krupski WC,
Busuttil SJ, Barone GW, Sparks S, Graham LM, Rapp JH, Makaroun MS,
Moneta GL, Cambria RA, Makhoul RG, Eton D, Ansel HJ, Freischlag
JA, Bandyk D. Immediate repair compared with surveillance of small
abdominal aortic aneurysms. N Engl J Med. 2002;346:1437–1444.
Coady MA, Rizzo JA, Hammond GL, Mandapati D, Darr U, Kopf GS,
Elefteriades JA. What is the appropriate size criterion for resection of
thoracic aortic aneurysms? J Thorac Cardiovasc Surg. 1997;113:
476 – 491.
Bickerstaff LK, Pairolero PC, Hollier LH, Melton LJ, Van Peenen HJ,
Cherry KJ, Joyce JW, Lie JT. Thoracic aortic aneurysms: a
population-based study. Surgery. 1982;92:1103–1108.
Crawford ES. Thoraco-abdominal and abdominal aortic aneurysms
involving renal, superior mesenteric, celiac arteries. Ann Surg. 1974;179:
763–772.
Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE Jr,
Eagle KA, Hermann LK, Isselbacher EM, Kazerooni EA, Kouchoukos
NT, Lytle BW, Milewicz DM, Reich DL, Sen S, Shinn JA, Svensson LG,
Williams DM. ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/
STS/SVM guidelines for the diagnosis and management of patients with
thoracic aortic disease: a report of the American College of Cardiology
Foundation/American Heart Association Task Force on Practice
Guidelines, American Association for Thoracic Surgery, American
College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and
Interventions, Society of Interventional Radiology, Society of Thoracic
Surgeons, and Society for Vascular Medicine. Circulation. 2010;121:
e266 – e369.
Bonow RO, Carabello B, de Leon AC Jr, Edmunds LH Jr, Fedderly BJ,
Freed MD, Gaasch WH, McKay CR, Nishimura RA, O’Gara PT,
O’Rourke RA, Rahimtoola SH, Ritchie JL, Cheitlin MD, Eagle KA,
Gardner TJ, Garson A Jr, Gibbons RJ, Russell RO, Ryan TJ, Smith SC Jr.
Guidelines for the management of patients with valvular heart disease:
executive summary: a report of the American College of Cardiology/
American Heart Association Task Force on Practice Guidelines (Committee
on Management of Patients with Valvular Heart Disease). Circulation. 1998;
98:1949–1984.
Conrad MF, Cambria RP. Contemporary management of descending
thoracic and thoracoabdominal aortic aneurysms: endovascular versus
open. Circulation. 2008;117:841– 852.
Achneck HE, Rizzo JA, Tranquilli M, Elefteriades JA. Safety of thoracic
aortic surgery in the present era. Ann Thorac Surg. 2007;84:1180 –1185.
Safi HJ, Estrera AL, Miller CC, Huynh TT, Porat EE, Azizzadeh A,
Meada R, Goodrick JS. Evolution of risk for neurologic deficit after
descending and thoracoabdominal aortic repair. Ann Thorac Surg. 2005;
80:2173–2179.
Svensson LG, Kouchoukos NT, Miller DC, Bavaria JE, Coselli JS, Curi
MA, Eggebrecht H, Elefteriades JA, Erbel R, Gleason TG, Lytle BW,
Mitchell RS, Nienaber CA, Roselli EE, Safi HJ, Shemin RJ, Sicard GA,
Sundt TM 3rd, Szeto WY, Wheatley GH 3rd. Expert consensus document
on the treatment of descending thoracic aortic disease using endovascular
stent-grafts. Ann Thorac Surg. 2008;85:S1–S41.
Bavaria JE, Appoo JJ, Makaroun MS, Verter J, Yu ZF, Mitchell RS.
Endovascular stent grafting versus open surgical repair of descending
thoracic aortic aneurysms in low-risk patients: a multicenter comparative
trial. J Thorac Cardiovasc Surg. 2007;133:369 –377.
Walsh SR, Tang TY, Sadat U, Naik J, Gaunt ME, Boyle JR, Hayes PD,
Varty K. Endovascular stenting versus open surgery for thoracic aortic
disease: systematic review and meta-analysis of perioperative results.
J Vasc Surg. 2008;47:1094 –1098.
Conrad MF, Ergul EA, Patel VI, Paruchuri V, Kwolek CJ, Cambria RP.
Management of diseases of the descending thoracic aorta in the endovascular era: a Medicare population study. Ann Surg. 2010;252:603– 610.
Medical Therapy of TAA
1475
53. Black SA, Wolfe JH, Clark M, Hamady M, Cheshire NJ, Jenkins MP.
Complex thoracoabdominal aortic aneurysms: endovascular exclusion
with visceral revascularization. J Vasc Surg. 2006;43:1081–1089.
54. Nienaber CA, Rousseau H, Eggebrecht H, Kische S, Fattori R, Rehders
TC, Kundt G, Scheinert D, Czerny M, Kleinfeldt T, Zipfel B, Labrousse
L, Ince H. Randomized comparison of strategies for type B aortic dissection: the INvestigation of STEnt Grafts in Aortic Dissection
(INSTEAD) trial. Circulation. 2009;120:2519 –2528.
55. Feldman M, Shah M, Elefteriades JA. Medical management of acute type
A aortic dissection. Ann Thorac Cardiovasc Surg. 2009;15:286 –293.
56. Karthikesalingam A, Holt PJ, Hinchliffe RJ, Thompson MM, Loftus IM.
The diagnosis and management of aortic dissection. Vasc Endovascular
Surg. 2010;44:165–169.
57. Gadowski GR, Pilcher DB, Ricci MA. Abdominal aortic aneurysm
expansion rate: effect of size and beta-adrenergic blockade. J Vasc Surg.
1994;19:727–731.
58. Leach SD, Toole AL, Stern H, DeNatale RW, Tilson MD. Effect of
beta-adrenergic blockade on the growth rate of abdominal aortic aneurysms. Arch Surg. 1988;123:606 – 609.
59. Shores J, Berger KR, Murphy EA, Pyeritz RE. Progression of aortic
dilatation and the benefit of long-term beta-adrenergic blockade in
Marfan’s syndrome. N Engl J Med. 1994;330:1335–1341.
60. Lindholt JS, Vammen S, Juul S, Henneberg EW, Fasting H. The validity
of ultrasonographic scanning as screening method for abdominal aortic
aneurysm. Eur J Vasc Endovasc Surg. 1999;17:472– 475.
61. Propranolol for small abdominal aortic aneurysms: results of a randomized trial. J Vasc Surg. 2002;35:72–79.
62. Nebivolol Versus Losartan Versus NebivololϩLosartan Against
Aortic Root Dilation in Genotyped Marfan Patients (MaNeLo). www.
clinicaltrials.gov. Identifier: NCT00683124. Accessed July 2011.
63. Petrinec D, Liao S, Holmes DR, Reilly JM, Parks WC, Thompson RW.
Doxycycline inhibition of aneurysmal degeneration in an elastaseinduced rat model of abdominal aortic aneurysm: preservation of aortic
elastin associated with suppressed production of 92 kD gelatinase. J Vasc
Surg. 1996;23:336 –346.
64. Hanemaaijer R, Sorsa T, Konttinen YT, Ding Y, Sutinen M, Visser H,
van Hinsbergh VW, Helaakoski T, Kainulainen T, Ronka H, Tschesche
H, Salo T. Matrix metalloproteinase-8 is expressed in rheumatoid
synovial fibroblasts and endothelial cells: regulation by tumor necrosis
factor-alpha and doxycycline. J Biol Chem. 1997;272:31504 –31509.
65. Xiong W, Knispel RA, Dietz HC, Ramirez F, Baxter BT. Doxycycline
delays aneurysm rupture in a mouse model of Marfan syndrome. J Vasc
Surg. 2008;47:166 –172.
66. Baxter BT, Pearce WH, Waltke EA, Littooy FN, Hallett JW Jr, Kent KC,
Upchurch GR Jr, Chaikof EL, Mills JL, Fleckten B, Longo GM, Lee JK,
Thompson RW. Prolonged administration of doxycycline in patients with
small asymptomatic abdominal aortic aneurysms: report of a prospective
(phase II) multicenter study. J Vasc Surg. 2002;36:1–12.
67. Mosorin M, Juvonen J, Biancari F, Satta J, Surcel HM, Leinonen M,
Saikku P, Juvonen T. Use of doxycycline to decrease the growth rate of
abdominal aortic aneurysms: a randomized, double-blind, placebocontrolled pilot study. J Vasc Surg. 2001;34:606 – 610.
68. Vammen S, Lindholt JS, Ostergaard L, Fasting H, Henneberg EW. Randomized double-blind controlled trial of roxithromycin for prevention of
abdominal aortic aneurysm expansion. Br J Surg. 2001;88:1066 –1072.
69. Sukhija R, Aronow WS, Sandhu R, Kakar P, Babu S. Mortality and size
of abdominal aortic aneurysm at long-term follow-up of patients not
treated surgically and treated with and without statins. Am J Cardiol.
2006;97:279 –280.
70. Ferguson CD, Clancy P, Bourke B, Walker PJ, Dear A, Buckenham T,
Norman P, Golledge J. Association of statin prescription with small
abdominal aortic aneurysm progression. Am Heart J. 2010;159:307–313.
71. Rizzoni D, Rodella L, Porteri E, Rezzani R, Sleiman I, Paiardi S, Guelfi
D, De Ciuceis C, Boari GE, Bianchi R, Agabiti-Rosei E. Effects of
losartan and enalapril at different doses on cardiac and renal interstitial
matrix in spontaneously hypertensive rats. Clin Exp Hypertens. 2003;25:
427– 441.
72. Nagashima H, Uto K, Sakomura Y, Aoka Y, Sakuta A, Aomi S, Hagiwara
N, Kawana M, Kasanuki H. An angiotensin-converting enzyme inhibitor,
not an angiotensin II type-1 receptor blocker, prevents betaaminopropionitrile monofumarate-induced aortic dissection in rats. J Vasc
Surg. 2002;36:818–823.
73. Brooke BS, Habashi JP, Judge DP, Patel N, Loeys B, Dietz HC 3rd.
Angiotensin II blockade and aortic-root dilation in Marfan’s syndrome.
N Engl J Med. 2008;358:2787–2795.
Downloaded from by guest on September 16, 2015
1476
Circulation
September 27, 2011
74. Hackam DG, Thiruchelvam D, Redelmeier DA. Angiotensin-converting
enzyme inhibitors and aortic rupture: a population-based case-control
study. Lancet. 2006;368:659 – 665.
75. Sweeting MJ, Thompson SG, Brown LC, Greenhalgh RM, Powell JT. Use of
angiotensin converting enzyme inhibitors is associated with increased growth
rate of abdominal aortic aneurysms. J Vasc Surg. 52:1–4.
76. Ahimastos AA, Aggarwal A, D’Orsa KM, Formosa MF, White AJ,
Savarirayan R, Dart AM, Kingwell BA. Effect of perindopril on large
artery stiffness and aortic root diameter in patients with Marfan syndrome: a randomized controlled trial. JAMA. 2007;298:1539 –1547.
77. Detaint D, Aegerter P, Tubach F, Hoffman I, Plauchu H, Dulac Y, Faivre
LO, Delrue MA, Collignon P, Odent S, Tchitchinadze M, Bouffard C,
Arnoult F, Gautier M, Boileau C, Jondeau G. Rationale and design of a
randomized clinical trial (Marfan Sartan) of angiotensin II receptor
blocker therapy versus placebo in individuals with Marfan syndrome.
Arch Cardiovasc Dis. 2010;103:317–325.
78. Golledge J, Muller J, Daugherty A, Norman P. Abdominal aortic aneurysm: pathogenesis and implications for management. Arterioscler
Thromb Vasc Biol. 2006;26:2605–2613.
79. Yoshimura K, Aoki H, Ikeda Y, Fujii K, Akiyama N, Furutani A, Hoshii
Y, Tanaka N, Ricci R, Ishihara T, Esato K, Hamano K, Matsuzaki M.
80.
81.
82.
83.
Regression of abdominal aortic aneurysm by inhibition of c-Jun
N-terminal kinase. Nat Med. 2005;11:1330 –1338.
Dobrin PB, Baumgartner N, Anidjar S, Chejfec G, Mrkvicka R. Inflammatory aspects of experimental aneurysms. Effect of methylprednisolone
and cyclosporine. Ann N Y Acad Sci. 1996;800:74 – 88.
Inoue N, Muramatsu M, Jin D, Takai S, Hayashi T, Katayama H, Kitaura
Y, Tamai H, Miyazaki M. Effects of chymase inhibitor on angiotensin
II-induced abdominal aortic aneurysm development in apolipoprotein
E-deficient mice. Atherosclerosis. 2009;204:359 –364.
Lindholt JS, Sorensen HT, Michel JB, Thomsen HF, Henneberg EW.
Low-dose aspirin may prevent growth and later surgical repair of
medium-sized abdominal aortic aneurysms. Vasc Endovascular Surg.
2008;42:329 –334.
Cornuz J, Sidoti Pinto C, Tevaearai H, Egger M. Risk factors for asymptomatic abdominal aortic aneurysm: systematic review and meta-analysis
of population-based screening studies. Eur J Public Health.
2004;14:343–349.
KEY WORDS: aneurysm Ⅲ aorta Ⅲ aortic aneurysm, abdominal
therapy Ⅲ aorta, thoracic Ⅲ aortic aneurysm, thoracic
Downloaded from by guest on September 16, 2015
Ⅲ
drug
Medical Therapy of Thoracic Aortic Aneurysms: Are We There Yet?
Peter Danyi, John A. Elefteriades and Ion S. Jovin
Circulation. 2011;124:1469-1476
doi: 10.1161/CIRCULATIONAHA.110.006486
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 2011 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
/>
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial
Office. Once the online version of the published article for which permission is being requested is located,
click Request Permissions in the middle column of the Web page under Services. Further information about
this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
/>Subscriptions: Information about subscribing to Circulation is online at:
/>
Downloaded from by guest on September 16, 2015