- Trang chủ >>
- Y - Dược >>
- Truyền nhiễm
Willingness to receive in the covid 19 vacine booster shot a case study from china
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (572.87 KB, 22 trang )
Click here to access/download;Figure;Figure 1.jpg
Figure 1
pr
no
int
tp
ev
ed
iew
ee
rr
This preprint research paper has not been peer reviewed. Electronic copy available at: />
Pr
e
Click here to access/download;Figure;Figure 2a.jpg
Figure 2a
pr
no
int
tp
ev
ed
iew
ee
rr
This preprint research paper has not been peer reviewed. Electronic copy available at: />
Pr
e
Click here to access/download;Figure;Figure 2b.jpg
Figure 2b
pr
no
int
tp
ev
ed
iew
ee
rr
This preprint research paper has not been peer reviewed. Electronic copy available at: />
Pr
e
Manuscript
Click here to view linked References
iew
ed
Willingness to receive the COVID-19 vaccine booster shot: a
cross-sectional study in China
Yongqing Deng1#, Xiaoqin Qiu2#, Caixian Huang3#, Weiwei Li4#, Liying Dai4#, Miaomiao Xie5,
Chaofeng Chen4, Runlin Han6, Yan Chen4, Shishan Huang7, Sujiao Qin2, Jiayin Ou8, Ting Shi9,
Li Zhang10, Yuechou Nong10, Jianrong Yang5, Wensheng Lu10*
rin
tn
ot
pe
er
re
v
1 The Family Planning Office, Guangxi Academy of Medical Sciences and the People’s
Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, 530021, P.R.China
2 The Nursing Department, Guangxi Academy of Medical Sciences and the People’s Hospital
of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, 530021, P.R.China
3 Department of Hematology, Guangxi Academy of Medical Sciences and the People’s
Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, 530021, P.R.China
4 The Office of Guangxi Academy of Medical Sciences and the People’s Hospital of Guangxi
Zhuang Autonomous Region, Nanning, Guangxi, 530021, P.R.China
5 Department of Hepatobiliary Surgery, Guangxi Academy of Medical Sciences and the
People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, 530021,
P.R.China
6 Guangxi University of Traditional Chinese Medicine, Nanning, Guangxi, 530021,
P.R.China
7 The Scientific Research Department, Guangxi Academy of Medical Sciences and the
People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, 530021,
P.R.China
8 Department of Medical Administration, Guangxi Academy of Medical Sciences and the
People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, 530021,
P.R.China
9 Department of Prevention and Health Care, Guangxi Academy of Medical Sciences and the
People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, 530021,
P.R.China
10 Department of Endocrinology and Metabolism, Guangxi Academy of Medical Sciences
and the People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi,
530021, P.R.China
Pr
ep
# They contributed equally to this work;
∗ Corresponding author: Prof. Wensheng Lu, E-mail: ; ORCID ID:
0000-0003-4179-1171
1
This preprint research paper has not been peer reviewed. Electronic copy available at: />
iew
ed
Summary
Background As the coronavirus disease 19 (COVID-19) global pandemic continues,
safe and effective vaccines and high vaccination coverage are still the most effective
way to the control of the COVID-19 epidemic. This study aimed to explore the
influencing factors of the willingness to receive the COVID-19 vaccine booster shot
in Chinese residents.
pe
er
re
v
Methods This was a cross-sectional study and a total of 1100 residents participated in
the anonymous questionnaire survey. The data collected included demographic
characteristics, residents’ awareness of COVID-19 epidemic, the attitude towards
COVID-19 vaccine and vaccination willingness. The multivariate logistic regression
analyses were used to assess the factors influencing the Chinese residents' willingness
to receive the COVID-19 vaccine booster shot.
Findings In total, 1006 valid questionnaires were collected with a response rate of
91.45%. Among them, 77.3% believed that the COVID-19 epidemic was serious, 88.8%
responded that the COVID-19 vaccine was safe and effective, 93.6% received the
two-dose COVID-19 vaccination and 86% were willing to receive COVID-19 vaccine
ot
booster shot. The concerns about vaccine safety were the main reason for willing to
the two-dose COVID-19 vaccination schedule and the COVID-19 vaccine booster
rin
tn
shot, accounting for 45% and 67%, respectively. Multivariate logistic regression
analyses revealed that male was less willingness to take COVID-19 vaccine booster
shot (OR = 0.630, 95%CI: 0.436 - 0.910, P = 0.014). But the residents of the 18 - 29
years of age group (OR = 2.708, 95%CI: 1.243 - 5.896, P = 0.012), the residents who
had received the two-dose COVID-19 vaccination (OR = 2.066, 95%CI: 1.120 - 3.811,
ep
P = 0.020) and who were afraid of being infected (OR =1.801, 95%CI: 1.230 - 2.638,
P = 0.002) were more willingness to take COVID-19 vaccine booster shot.
Interpretation Most residents were willing to receive the COVID-19 vaccine booster
Pr
shot. Being female, younger age and the residents who had received the two-dose
COVID-19 vaccination and who were afraid of being infected were statistically
significantly associated with willingness to receive COVID-19 vaccine booster shot.
2
This preprint research paper has not been peer reviewed. Electronic copy available at: />
iew
ed
Fundings Natural Science Foundation of China (81560044, 30860113, 82160052),
Guangxi Medical and Health Appropriate Technology Research and Development
Project (S201315-03, S201422-01), Guangxi Zhuang Autonomous Region Health
Committee Project (Z20190209), Shanxi Health Research Project (2019165).
Introduction
pe
er
re
v
Corona Virus Disease 2019 (COVID-19) is an emerging infectious disease caused by
a novel corona virus, Severe Acute Respiratory Coronavirus 2 (SARS-COV-2). It is a
global pandemic that has seriously threatened human health and has hindered
socio-economic development.1,2 As of October 2021, the cumulative number of
confirmed COVID-19 cases worldwide has exceeded 240 million, with more than 4.9
million deaths. For most countries, developing a safe and effective vaccine is urgently
required to protect against the COVID-19 pandemic, and a total of more than 6.6
billion doses of COVID-19 vaccine have been received.3 Currently, 275 COVID-19
vaccine candidates are being tested around the world and 24 of these have been
approved. In China, four COVID-19 vaccines have been approved for marketing.4
ot
However, vaccine-induced levels of neutralizing antibody are decreasing over time
and then the protective efficacy is declined. In this situation, the increase in the
rin
tn
vaccination number is to provide long-lasting immunity.5,6 The Israeli study7,8 showed
that people who received the COVID-19 vaccine booster shot had a lower rate
ofsevere illness by a factor of 19.5. Recently, China has taken COVID-19 vaccination
programs of a booster shot, and people aged 18 or over who have received two dose
of COVID-19 vaccination can receive a booster dose.9
ep
The COVID-19 vaccine acceptance varies across the world. About 81.1% of
Chinese were willing to take the vaccine before mass vaccination.10,11,12,13 A study in
the United States14 found that the COVID-19 vaccination rate dropped from 74% to
Pr
56%, which may be related to low educational background. A community-based study
in India found that about 19.5% of residents refused to be vaccinated and 40.7% of
residents had vaccine hesitancy.15 Improving vaccination coverage is the key to
3
This preprint research paper has not been peer reviewed. Electronic copy available at: />
iew
ed
controlling the COVID-19 pandemic,16,17 but vaccine hesitancy is the main factor
affecting vaccination coverage.18,19 Therefore, it is very important to know whether
people are willing to receive the COVID-19 vaccine booster shot, which can develop
an effective strategy to facilitate COVID-19 vaccine booster shot rollout.
Therefore, we conducted a cross-sectional study to assess Chinese residents’
attitude, acceptance to receive the COVID-19 vaccine booster shot, and influencing
factors associated with Chinese residents’ willingness to receive the COVID-19
pe
er
re
v
vaccine booster shot. To our knowledge, it is the first cross-sectional study for
willingness to receive the COVID-19 vaccine booster shot based on Chinese
population.
Methods
Survey design
The cross-sectional study was conducted from July 20, 2021 to September 30, 2021.
We conducted an anonymous questionnaire survey of 1,100 residents aged 18 years or
above who have received the two-dose COVID-19 vaccination in 5 communities
ot
including the Forestry Academy, Beihu, Lianchou, Xijin, and Yongning, Guangxi
Province, China. We excluded those who had difficulties in listening, speaking,
rin
tn
understanding and communication, and those who were unable to complete the
questionnaire due to mental illness. All participants voluntarily participated in this
study and signed an informed consent form before inclusion in this study. This study
was approved by the Ethics Committee of the People’s Hospital of Guangxi Zhuang
Autonomous Region.
ep
Sample size estimation
We used the Cochran formula20 to estimate the sample size: n = z2pq/e2 =1.962 × 0.5
(1-0.5)/0.052 = 384. Where, n = sample size, z = 1.96 [95% confidence interval (CI)],
Pr
p = an estimated incidence rate (50%), q = (1- p), e = the absolute allowable error
(5%). Assuming a 10% non-response rate, the total sample size is 423.5 ≈ 424. Our
sample size is larger than this estimate.
4
This preprint research paper has not been peer reviewed. Electronic copy available at: />
iew
ed
Survey design
According to the published literature21,22 and the actual situation, we designed the
questionnaire with four main sections: (1) demographic characteristics; (2) the
cognition of COVID-19 epidemic situation; (3) the attitudes towards COVID-19
vaccine;
(4)
willingness
to
receive
COVID-19
vaccination.
Demographic
characteristics comprised 10 items, including gender, age group, place of residence,
marital status, education level, medical insurance type, monthly income, occupation,
pe
er
re
v
whether they suffer from chronic diseases, and whether they have received other
vaccinations in the past year. The questionnaire about residents’ awareness of the
COVID-19 epidemic had 7 items, including infection risk, severity of the outbreak,
and the impact of the COVID-19 outbreak on quality of life. The third section
discussed about residents’ attitudes towards the COVID-19 vaccine, including
concerns about vaccine safety. Vaccination intentions included the willingness or
unwillingness to take COVID-19 vaccine booster shot, the reasons for unwillingness
(sub-item), whether you have received the two-dose COVID-19 vaccination, the
reasons for not completing the two-dose COVID-19 vaccination (sub-item) and the
Quality control
ot
reluctance to receive COVID-19 vaccine booster shot.
rin
tn
The anonymous questionnaire survey was conducted by professionally trained
investigators. The participants were selected in accordance with the strict inclusion
and exclusion criteria. The relevant basic information was collected, then the
participants were given questionnaires and were asked to fill in the questionnaire as
completely and accurately as possible. After the questionnaire was completed, the
investigators would check the questionnaire in time and erroneous or inconsistent data
ep
were excluded to ensure the reliability of the data.
Statistical analysis
Pr
All statistical analyses were performed using IBM Statistical Package for the Social
Sciences software (SPSS Version 21, IBM, Chicago, USA). Descriptive statistics were
calculated as frequency, percentage, mean, standard deviation (SD). The one-way
analysis of variance was used to examine the relationship between variables and the
5
This preprint research paper has not been peer reviewed. Electronic copy available at: />
iew
ed
COVID-19 vaccination. The multivariate logistic regression model was applied to
analyze the influencing factors of the willingness to take the COVID-19 vaccine
booster shot and the statistically significant variables (P value < 0.1) in the one-way
ANOVA were further enrolled into the multivariate logistic regression analysis. P
value < 0.05 was considered statistically significant.
pe
er
re
v
Results
In this study, a total of 1006 valid questionnaires were collected with an effective
response rate of 91.45% (1006/1100). The demographic characteristics of survey
respondents were shown in the Table 1. The majority of the respondents were female
(54.4%), married (83.3%), were in the age group 30 - 39 years (36.4%) and lived in
rural areas (58.9%). The educational level of the present samples was mainly junior
high school (48.8%). The majority of the group were migrant workers (61.7%) and
47.5% had monthly incomes of less than 3000 RMB. Besides, 62.9% have rural
insurance, 94% had no chronic disease and 99.1% hadn’t received other vaccines in
the past year.
ot
In terms of survey responses, the data revealed that 61.5% (619/1006) of residents
agreed or strongly agreed that they were at high risk of contracting the COVID-19,
rin
tn
and 77.3% (778/1006) believed that the COVID-19 epidemic was serious. Of these,
41.6% (418/1006) believed that the COVID-19 epidemic continues to spread, but 41.3%
disagreed or strongly disagreed that the COVID-19 epidemic would rebound. Most
residents (678/1006 (67.4%)) took the initiative to focus on the updated data about the
COVID-19 epidemic at home and abroad. In addition, 67.4% (678/1006) agreed or
ep
strongly agreed that the quality of life was severely affected by the COVID-19
epidemic in the past year. About 35.3% (355/1006) indicated that the quality of life
would be severely affected by the COVID-19 epidemic in the next year, however,
Pr
47.3% (476/1006) remained neutral (Table 2).
We used four questions to assess the residents' attitudes towards the COVID-19
vaccine and the results were listed in the Table 3. A total of 893 residents (893/1006
6
This preprint research paper has not been peer reviewed. Electronic copy available at: />
iew
ed
(88.8%)) agreed or strongly agreed that the COVID-19 vaccine was safe and effective,
89% (895/1006) also agree or strongly agreed that the COVID-19 epidemic can be
effectively prevented by vaccination. Among them, 84% (845/1006) believed that
there were differences between domestic and imported vaccines, and 84.9%
(854/1006) strong agreed that they can accept self-paid vaccine.
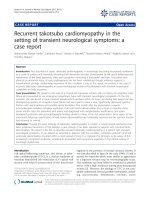
Among the residents surveyed, 942 (93.6%) received the two-dose COVID-19
vaccination, and 64 (6.4%) did not received it. In the meanwhile, the results indicated
were unwilling (Figure 1).
pe
er
re
v
that 865 (86%) were willing to receive COVID-19 vaccine booster shot, only 14%
According to our survey, the concerns about vaccine safety was the main reason for
the two-dose COVID-19 vaccination schedule, accounting for 45%, followed by
pregnancy, lactation and work trip, accounting for 42% and 13%, respectively (Figure
2a). Besides, concerns about vaccine safety were also the major reason accounting for
residents’ unwillingness to receive the COVID-19 vaccine booster shot, accounting
for 67%, followed by pregnancy and lactation and contraindications for vaccination,
accounting for 21% and 12% respectively (Figure 2b).
ot
The results showed that gender and age were significantly associated with the
willingness to receive the COVID-19 vaccine booster shot (both P < 0.05). Moreover,
rin
tn
most residents were willing to receive the two-dose COVID-19 vaccination (P =
0.021). However, they hadn't received the COVID-19 vaccine booster shot yet
because of fear of infection (P = 0.001). The residents who obtained information
about COVID-19 vaccine booster shot through various ways were more willing to be
vaccinated (P = 0.026) (Table 4).
A multivariate logistic regression model was used to analyze the relevant factors of
ep
the willingness to take the COVID-19 vaccine booster shot and the statistically
significant variables in the one-way analysis of variance were included. The results
Pr
showed that male, age, and the residents who had received the two-dose COVID-19
vaccination or were afraid of being infected were statistically significantly associated
with willingness to receive COVID-19 vaccine booster shot. Specifically, male was
less willingness to take COVID-19 vaccine booster shot (OR = 0.630, 95%CI: 0.436 7
This preprint research paper has not been peer reviewed. Electronic copy available at: />
iew
ed
0.910, P = 0.014). But the residents of the 18 - 29 years of age group (OR = 2.708,
95%CI: 1.243 - 5.896, P = 0.012), the residents who had received the two-dose
COVID-19 vaccination (OR = 2.066, 95%CI: 1.120 - 3.811, P = 0.020) and who
were afraid of being infected (OR =1.801, 95%CI: 1.230 - 2.638, P = 0.002) were
more willingness to take COVID-19 vaccine booster shot (Table 5).
pe
er
re
v
Discussion
The COVID-19 pandemic has posed unprecedented burdens to healthcare systems
worldwide, and COVID-19 vaccination is considered to be the most effective
intervention to control the pandemic. The success of the vaccination schedule depends
on the vaccination coverage rate,23 but vaccine hesitancy is the major factor affecting
the coverage rate of COVID-19 vaccination.18 As a result, understanding the
willingness and influencing factors of COVID-19 vaccination is uniquely important
and can guide effective measures to fight the COVID-19 pandemic.24,25 To date, few
study explored Chinese residents’ willingness to receive the COVID-19 vaccine
booster shot. As far as we know, it is the first cross-sectional study for willingness to
ot
receive the COVID-19 vaccine booster shot based on Chinese population. In our study,
77.3% of residents believed that the COVID-19 epidemic was serious, 88.8% agreed
rin
tn
or strongly agreed that the COVID-19 vaccine was safe and effective and 89%
thought that the COVID-19 epidemic can be effectively prevented by vaccination.
Next, we found that 93.6% received the two-dose COVID-19 vaccination and 86%
were willing to receive COVID-19 vaccine booster shot. The results of one-way
ANOVA showed that gender and age were significantly associated with the
ep
willingness to receive the COVID-19 vaccine booster shot, most residents were
willing to receive the two-dose COVID-19 vaccination. However, they haven't
received the COVID-19 vaccine booster shot yet because of fear of infection. The
Pr
residents who obtained information about COVID-19 vaccine booster shot through
various ways were more willing to be vaccinated. Multivariate logistic regression
analyses revealed that male was less willingness to take COVID-19 vaccine booster
8
This preprint research paper has not been peer reviewed. Electronic copy available at: />
iew
ed
shot. But the residents of the 18 - 29 years of age group, the residents who had
received the two-dose COVID-19 vaccination or were afraid of being infected were
more willingness to take COVID-19 vaccine booster shot.
We found that the participants had a positive attitude towards the COVID-19
vaccine. Although the COVID-19 epidemic is considered a serious health concern
worldwide, they believed COVID-19 vaccine was safe and effective and can
effectively prevent the COVID-19 epidemic. We found that the majority of Chinese
pe
er
re
v
residents had received the two dose of COVID-19 vaccine and were willing to receive
COVID-19 vaccine booster shot, which was within the similar range as the studies by
Lazarus et al.26 and Dodd et al..27 Lazarus et al found that 86.6% (631/712)
respondents from China were willing to take the COVID-19 vaccine. Dodd et al.
reported that 85.8% (3741/4362) participants would accept the vaccine if the
COVID-19 vaccine was available. These results suggested that the willingness to get
vaccinated against COVID-19 was strong for general public. Currently, public
concerns about vaccine safety increases the risk of vaccination hesitancy and affect
the high vaccine coverage.28 In our survey, the concerns about vaccine safety were the
ot
main reason accounting for residents’ unwillingness to receive the COVID-19
vaccination schedule. Hence, in practical work, the government should increase
rin
tn
advocacy to let the general public know about the hazards of COVID-19, the
therapeutic and preventive interventions of the COVID-19 and the protective effect of
the COVID-19 vaccine. Additionally, the channels and forms of publicity should be
diverse, the coverage should be wide and the false and negative publicity should be
verified and corrected.29,30 These will strengthen residents’ awareness of the necessity
of the COVID-19 vaccination and enhance confidence in vaccination against
ep
COVID-19.
Furthermore, we investigated the factors influencing the Chinese residents'
Pr
willingness to receive the COVID-19 vaccine booster shot. We found that female was
more likely to receive COVID-19 vaccine booster shot than male. This is consistent
with the previous studies.31,32 Then, we reported that younger people tended to be
willingness to receive COVID-19 vaccine booster shot. This is contradicted with other
9
This preprint research paper has not been peer reviewed. Electronic copy available at: />
iew
ed
studies31,33 and we considered the possible reasons as follows. First, there are gender
differences between countries in terms of vaccination willingness. Second, with the
COVID-19 vaccine knowledge promotion, vaccination promotion, the protective
efficacy and less side effects of vaccine being confirmed, younger people had a better
understanding of the COVID-19 vaccine and therefore might be more willing to
receive the COVID-19 vaccine booster shot. Further study reported that the residents
had
received
the
were afraid of being infected
two
dose
of
were
statistically
COVID-19
significantly
vaccine
or
who
associated
with
pe
er
re
v
who
willingness to receive COVID-19 vaccine booster shot. The protective efficacy and
less side effects of vaccine were validated and thus it was more acceptable to be
vaccinated against COVID-19. The widespread anxiety and psychological problems
caused by the pandemic affect poor health perceptions.34,35,36 As the promotion of the
COVID-19 vaccine, they were more intent to be vaccinated against COVID-19 and
anxiety was considered to relieved.
This study still has some shortcomings. First of all, the sample size was relatively
small and our study was conducted at a single location; hence, a larger sample size
ot
and multi-sites are needed for further study. Next, due to the nature of the
cross-sectional design, the conclusions were regarded as associations rather than
rin
tn
causal relationships. However, the results and suggestions of this study have potential
application value for policy makers.
In summary, most residents were willing to receive the COVID-19 vaccine booster
shot. Being female, younger age and the residents who had received the two-dose
COVID-19 vaccination and who were afraid of being infected were statistically
significantly associated with willingness to receive COVID-19 vaccine booster shot.
ep
This study will provide reliable and important information to help policy makers
Pr
make an effective vaccination strategy.
Ethics approval and consent to participate
All patients agreed to participate in this study and signed written informed consent. The guidelines
outlined in the Declaration of Helsinki were followed. All survey were performed with approval
10
This preprint research paper has not been peer reviewed. Electronic copy available at: />
iew
ed
from the Ethics Committee of the Peoples Hospital of Guangxi Zhuang Autonomous Region.
Contributions
All authors contributed to data analysis, drafting or revising the manuscript. All authors read and
approved the final manuscript and agree to be accountable for all aspects of the work. Wensheng
Lu is the guarantor of this work and, as such, had full access to all the data in the study and takes
responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of interests
pe
er
re
v
The authors declare that they have no known competing financial interests or personal
relationships that could have appeared to influence the work reported in this paper.
Data and resource availability
The corresponding author has full access to all data in the study and is ultimately responsible for
the decision to submit this manuscript for publication.
Acknowledgements
The authors would like to thank the participants for their contributions to the survey. Thanks to
Baohui Xie, Yuanlin Huang, Qiufeng Yan, Jining Wei, Qiuhua Lu, Binbin Chen, Jinxu Liang,
ot
Qiuyun Nong, Chaozan Yang, Yongguang Su for collecting data.
References
1 Liu X, Shaw RH, Stuart ASV, et al. Safety and immunogenicity of heterologous versus homologous
rin
tn
prime-boost schedules with an adenoviral vectored and mRNA COVID-19 vaccine (Com-COV): a
single-blind, randomised, non-inferiority trial. Lancet 2021; 398(10303): 856-869.
2 Ramasamy MN, Minassian AM, Ewer KJ, et al. Safety and immunogenicity of ChAdOx1 nCoV-19
vaccine administered in a prime-boost regimen in young and old adults (COV002): a single-blind,
randomised, controlled, phase 2/3 trial. Lancet 2021; 396(10267): 1979-1993.
3 World Health Organization . WHO Coronavirus Disease (COVID-19) Dashboard (2021). Available at:
/>4
Milken
Institute’s
COVID-19
Treatment
and
Vaccine
Tracker.
Available
online:
ep
/>
5 Krause PR, Fleming TR, Peto R, et al. Considerations in boosting COVID-19 vaccine immune
responses. Lancet. Oct 9 2021;398(10308):1377-1380.
6 Shaw RH, Stuart A, Greenland M, Liu X, Nguyen Van-Tam JS, Snape MD; Com-COV Study Group.
Pr
Heterologous prime-boost COVID-19 vaccination: initial reactogenicity data. Lancet 2021;
397(10289): 2043-2046.
7 Mahase E. Covid-19: Booster dose reduces infections and severe illness in over 60s, Israeli study
reports. BMJ 2021; 374: n2297.
11
This preprint research paper has not been peer reviewed. Electronic copy available at: />
8 Kozlov M. COVID-vaccine booster shot shows promise in Israeli study. Nature 2021; 16.
iew
ed
9 Li G, Yi B, Liu J, et al. Effect of CYP3A4 Inhibitors and Inducers on Pharmacokinetics and
Pharmacodynamics of Saxagliptin and Active Metabolite M2 in Humans Using Physiological-Based
Pharmacokinetic Combined DPP-4 Occupancy. Front Pharmacol 2021; 12: 746594.
10 Wang C, Han B, Zhao T, et al. Vaccination willingness, vaccine hesitancy, and estimated coverage at
the first round of COVID-19 vaccination in China: A national cross-sectional study. Vaccine 2021;
39(21): 2833-2842.
11 Kukreti S, Lu MY, Lin YH, et al. Willingness of Taiwan's Healthcare Workers and Outpatients to
Vaccinate against COVID-19 during a Period without Community Outbreaks. Vaccines (Basel) 2021;
9(3).
pe
er
re
v
12 Chen M, Li Y, Chen J, Wen Z, Feng F, Zou H, Fu C, Chen L, Shu Y, Sun C. An online survey of the
attitude and willingness of Chinese adults to receive COVID-19 vaccination. Hum Vaccin
Immunother 2021 Jul 3; 17(7): 2279-2288.
13 Gan L, Chen Y, Hu P, Wu D, Zhu Y, Tan J, Li Y, Zhang D. Willingness to Receive SARS-CoV-2
Vaccination and Associated Factors among Chinese Adults: A Cross Sectional Survey. Int J Environ
Res Public Health 2021; 18(4): 1993.
14 Szilagyi PG, Thomas K, Shah MD, et al. National Trends in the US Public's Likelihood of Getting a
COVID-19 Vaccine-April 1 to December 8, 2020. JAMA 2020.
15 Danabal KGM, Magesh SS, Saravanan S, Gopichandran V. Attitude towards COVID 19 vaccines
and vaccine hesitancy in urban and rural communities in Tamil Nadu, India - a community based
survey. BMC Health Serv Res 2021; 21(1): 994.
16 Haas EJ, Angulo FJ, McLaughlin JM, et al. Impact and effectiveness of mRNA BNT162b2 vaccine
against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a
nationwide vaccination campaign in Israel: an observational study using national surveillance data.
Lancet 2021; 397(10287): 1819-1829.
ot
17 Haas EJ, McLaughlin JM, Khan F, et al. Infections, hospitalisations, and deaths averted via a
nationwide vaccination campaign using the Pfizer-BioNTech BNT162b2 mRNA COVID-19 vaccine
in Israel: a retrospective surveillance study. Lancet Infect Dis 2021; 22: S1473-3099(21)00566-1.
rin
tn
18 Graffigna G, Palamenghi L, Boccia S, Barello S. Relationship between Citizens' Health Engagement
and Intention to Take the COVID-19 Vaccine in Italy: A Mediation Analysis. Vaccines (Basel) 2020;
8(4).
19 Barello S, Nania T, Dellafiore F, Graffigna G, Caruso R. 'Vaccine hesitancy' among university
students in Italy during the COVID-19 pandemic. Eur J Epidemiol 2020; 35(8): 781-783.
20 Dell RB, Holleran S, Ramakrishnan R. Sample size determination. ILAR J 2002; 43(4): 207-13.
21 Zewude B, Belachew A. Intention to Receive the Second Round of COVID-19 Vaccine Among
Healthcare Workers in Eastern Ethiopia. Infect Drug Resist 2021; 14: 3071-3082.
ep
22 Schwarzinger M, Watson V, Arwidson P, Alla F, Luchini S. COVID-19 vaccine hesitancy in a
representative working-age population in France: a survey experiment based on vaccine
characteristics. Lancet Public Health 2021; 6(4): e210-e221.
23 Nuno M, Chowell G, Gumel AB. Assessing the role of basic control measures, antivirals and
Pr
vaccine in curtailing pandemic influenza: scenarios for the US, UK and the Netherlands. J R Soc
Interface 2007; 4(14): 505-21.
24 Han K, Francis MR, Zhang R, et al. Confidence, Acceptance and Willingness to Pay for the
COVID-19 Vaccine among Migrants in Shanghai, China: A Cross-Sectional Study. Vaccines (Basel)
12
This preprint research paper has not been peer reviewed. Electronic copy available at: />
2021; 9(5).
self-paid vaccines in China. Vaccine 2014; 32(35): 4471-4477.
iew
ed
25 Hou Z, Jie Chang, Yue D, Fang H, Meng Q, Zhang Y. Determinants of willingness to pay for
26 Lazarus JV, Ratzan SC, Palayew A, et al. A global survey of potential acceptance of a COVID-19
vaccine. Nat Med 2021; 27(2): 225-228.
27 Dodd RH, Cvejic E, Bonner C, Pickles K, McCaffery KJ, Sydney Health Literacy Lab C-g.
Willingness to vaccinate against COVID-19 in Australia. Lancet Infect Dis 2021; 21(3): 318-319.
28 Baxter R, Klein NP. Kaiser Permanente Vaccine Study Center: Highlights of 2009-2012. Vaccines
(Basel) 2013; 1(2): 139-53.
29 Basch CH, Zybert P, Reeves R, Basch CE. What do popular YouTube(TM) videos say about
pe
er
re
v
vaccines? Child Care Health Dev 2017; 43(4): 499-503.
30 Chan C, Sounderajah V, Daniels E, Acharya A, Clarke J, Yalamanchili S, Normahani P, Markar S,
Ashrafian H, Darzi A. The Reliability and Quality of YouTube Videos as a Source of Public Health
Information Regarding COVID-19 Vaccination: Cross-sectional Study. JMIR Public Health Surveill
2021; 7(7): e29942.
31 Diesel J, Sterrett N, Dasgupta S, et al. COVID-19 Vaccination Coverage Among Adults - United
States, December 14, 2020-May 22, 2021. MMWR Morb Mortal Wkly Rep 2021; 70(25): 922-927.
32 Murthy BP, Sterrett N, Weller D, Zell E, Reynolds L, Toblin RL, Murthy N, Kriss J, Rose C,
Cadwell B, Wang A, Ritchey MD, et al. Disparities in COVID-19 Vaccination Coverage Between
Urban and Rural Counties - United States, December 14, 2020-April 10, 2021.
33 Neumann-Bohme S, Varghese NE, Sabat I, et al. Once we have it, will we use it? A European survey
on willingness to be vaccinated against COVID-19. Eur J Health Econ 2020; 21(7): 977-982.
34 Chou WS, Budenz A. Considering Emotion in COVID-19 Vaccine Communication: Addressing
Vaccine Hesitancy and Fostering Vaccine Confidence. Health Commun 2020; 35(14): 1718-1722.
35 Mosby I, Swidrovich J. Medical experimentation and the roots of COVID-19 vaccine hesitancy
ot
among Indigenous Peoples in Canada. CMAJ 2021; 193(11): E381-E383.
36 Cooper S, van Rooyen H, Wiysonge CS. COVID-19 vaccine hesitancy in South Africa: how can we
Pr
ep
rin
tn
maximize uptake of COVID-19 vaccines? Expert Rev Vaccines 2021; 20(8): 921-933.
13
This preprint research paper has not been peer reviewed. Electronic copy available at: />
Table 1 Demographic characteristics of survey respondents (N = 1006)
Number of individuals (n)
Gender
Male
459
Female
547
Age group (years)
159
30 - 39
366
40 - 49
243
50 - 59
149
≥60
89
pe
er
re
v
18 - 29
Weighted (%)
iew
ed
Variable
Place of residence
Urban
Rural
Marital status
Married
Unmarried
Other
Education level
Elementary school and below
45.6
54.4
15.8
36.4
24.2
14.8
8.8
413
41.1
593
58.9
838
83.3
129
12.8
39
3.9
94
9.3
491
48.8
227
22.6
194
19.3
633
62.9
355
35.3
18
1.8
0 - 3000
478
47.5
3001 - 6000
374
37.2
6001 - 9000
109
10.8
≥9001
45
4.5
98
9.7
Migrant workers
621
61.7
Teacher
34
3.4
Medical staff
23
2.3
Freelance
230
22.9
Junior high school
High school
University and above
Medical insurance type
Urban insurance
Self-paid
rin
tn
Monthly income (RMB)
ot
Rural insurance
Occupation
ep
Personnel of enterprises and institutions
Suffer from chronic diseases
60
6
No
946
94
Yes
9
0.9
No
997
99.1
Pr
Yes
Have received other vaccines in the past year
14
This preprint research paper has not been peer reviewed. Electronic copy available at: />
iew
ed
Table 2 Residents' awareness of the COVID-19 epidemic
Strongly
Question
Strongly
Disagree, n
Neutral, n
Agree, n
(%)
(%)
(%)
Disagree, n
Agree, n
(%)
contracting the COVID-19?
Do you agree that the COVID-19 epidemic is
serious?
Do you agree that the COVID-19 epidemic
continues to spread?
Do you agree that the COVID-19 epidemic will
rebound?
Do you agree that you often focus on the updated
data about the COVID-19 epidemic at home and
abroad?
Do you agree that your quality of life has been
severely affected by the COVID-19 epidemic in
the past year?
Do you agree that your quality of life will be
severely affected by the COVID-19 epidemic in
116
267
513
106
(0.4%)
(11.6%)
(26.5%)
(51.0%)
(10.5%)
4
45
179
518
260
(0.4%)
(4.5%)
(17.8%)
(51.5%)
(25.8%)
22
243
323
366
52
(2.2%)
(24.1%)
(32.1%)
(36.4%)
(5.2%)
60
355
311
253
27
(6.0%)
(35.3%)
(30.9%)
(25.1%)
(2.7%)
8
70
250
583
95
(0.8%)
(6.9%)
(24.9%)
(58.0%)
(9.4%)
1
92
362
442
109
(0.1%)
(9.2%)
(36.0%)
(43.9%)
(10.8%)
12
163
476
301
54
(1.2%)
(16.2%)
(47.3%)
(29.9%)
(5.4%)
Pr
ep
rin
tn
ot
the next year?
4
pe
er
re
v
Do you agree that you are at high risk of
(%)
15
This preprint research paper has not been peer reviewed. Electronic copy available at: />
Table 3 Residents' attitudes towards the COVID-19 vaccine
Question
Strongly
Disagree,
Neutral, n
Agree, n
n (%)
(%)
(%)
Disagree,
Agree, n
n (%)
(%)
0
10
103
748
145
(0%)
(1.0%)
(10.2%)
(74.4%)
(14.4%)
1
9
101
744
151
(0.1%)
(0.9%)
(10.0%)
(74.0%)
(15.0%)
2
118
21
845
20
(0.2%)
(11.7%)
(2.1%)
(84.0%)
(2.0%)
2
7
25
118
854
Do you believe that the COVID-19 vaccine is safe and effective?
Do you agree that the COVID-19 epidemic can be effectively
prevented by vaccination?
Do you agree that there are differences between domestic and
Do you think that you can accept self-paid vaccine?
pe
er
re
v
imported vaccines?
iew
ed
Strongly
(0.7%)
(2.5%)
(11.7%)
(84.9%)
Pr
ep
rin
tn
ot
(0.2%)
16
This preprint research paper has not been peer reviewed. Electronic copy available at: />
iew
ed
Table 4 Results of one-way ANOVA for willingness to take COVID-19 vaccine booster shot
Unwilling or
Category
Willing, n (%)
P value
undecided, n (%)
Gender
0.014*
Male
381 (83.0%)
Female
484 (88.5%)
Age group (years)
78 (17.0%)
63 (11.5%)
0.038*
146 (91.8%)
30 - 39
312 (85.2%)
40 - 49
213 (87.7%)
50 - 59
124 (83.2%)
13 (8.2%)
54 (14.8%)
30 (12.3%)
25 (16.8%)
pe
er
re
v
18 - 29
≥60
70 (78.7%)
Place of residence
City
Rural area
Marital status
Married
Unmarried
Other
Education level
Elementary school and below
Junior high school
High school
University and above
19 (21.3%)
359 (86.9%)
54 (13.1%)
506 (85.3%)
87 (14.7%)
716 (85.4%)
122 (143.6%)
115 (89.1%)
14 (10.9%)
34 (87.2%)
5 (12.8%)
77 (81.9%)
17 (18.1%)
416 (84.7%)
75 (15.3%)
195 (85.9%)
32 (14.1%)
177 (91.2%)
17 (8.8%)
Rural medical insurance
City Medical Insurance
rin
tn
Own expense
0.517
0.095
0.840
ot
Medical insurance
0.474
542 (85.6%)
91 (14.4%)
308 (86.6%)
47 (13.2%)
15 (83.3%)
3 (16.7%)
Monthly income (RMB)
0.144
0 - 3000
403 (84.3%)
75 (15.7%)
3001 - 6000
327 (87.4%)
47 (12.6%)
6001 - 9000
92 (84.4%)
17 (15.6%)
≥9001
43 (95.6%)
2 (4.4%)
Profession
0.361
80 (81.6%)
18 (18.4%)
Migrant workers
533 (85.8%)
88 (14.2%)
ep
Personnel of government agencies and Institutions
Teacher
28 (82.4%)
6 (17.6%)
Medical staff
22 (95.7%)
1 (4.3%)
Freelance
202 (87.8%)
28 (12.2%)
0.142
Pr
Suffer from chronic diseases
Yes
47 (78.3%)
13 (21.7%)
No
818 (86.5%)
128 (13.5%)
Have you received other vaccines in the past year?
0.801
17
This preprint research paper has not been peer reviewed. Electronic copy available at: />
8 (88.9%)
1 (11.1%)
No
857 (86.0%)
140 (14.0%)
Have you received the two-dose COVID-19 vaccination?
iew
ed
Yes
0.021*
Yes
818 (86.8%)
No
47 (73.4%)
Fear of infection
124 (13.2%)
17 (26.6%)
0.001*
Yes
638 (88.5%)
No
227 (79.6%)
Ways to obtain information about COVID-19 vaccine booster shot
58 (20.4%)
0.026*
28 (87.5%)
4 (12.5%)
pe
er
re
v
Television
83 (11.5%)
Internet
Cell phone
Community promotion
Other
94 (81.7%)
21 (18.3%)
272 (90.7%)
28 (9.3%)
339 (82.9%)
70 (17.1%)
132 (88.0%)
18 (12.0%)
The vaccination form of COVID-19 vaccine booster shot
Unit organization
Community organization
Online appointment
On-site hospital appointment
Other
2 (8.3%)
108 (85.7%)
18 (14.3%)
215 (88.1%)
29 (11.9%)
367 (84.2%)
69 (15.8%)
153 86.9%)
23 (13.1%)
Pr
ep
rin
tn
ot
*P < 0.05
22 (91.7%)
0.578
18
This preprint research paper has not been peer reviewed. Electronic copy available at: />
Table 5 Results of the multivariate logistic regression analysis for willingness to take COVID-19 vaccine booster shot
OR
95% CI
P value
Male
0.63
(0.436 - 0.910)
0.014*
Female
1.00
-
-
iew
ed
Influencing factors
Gender
Age group (years)
0.076
2.708
(1.243 - 5.896)
0.012*
30 - 39
1.326
(0.726 - 2.424)
0.358
40 - 49
1.631
(0.847 - 3.140)
0.143
50 - 59
1.101
(0.554 - 2.187)
0.783
≥60
1.00
-
-
2.066
(1.120 - 3.811)
0.020*
1.00
-
-
1.801
(1.230 - 2.638)
0.002*
1.00
-
-
Have you received the two-dose COVID-19 vaccination?
Yes
No
Fear of infection
Yes
No
Ways to obtain information about COVID-19 vaccine booster shot
Television
Internet
Cell phone
Community promotion
Other
pe
er
re
v
18 - 29
0.063
0.997
(0.307 - 3.233)
0.996
0.653
(0.325 - 1.310)
0.230
1.327
(0.701 - 2.511)
0.384
0.688
(0.391 - 1.212)
0.195
1.00
-
-
rin
tn
Figure legends
ot
OR: odds ratio; 95% CI: 95% confidence interval; *P < 0.05.
Figure 1: The completion of the two-dose COVID-19 vaccination and the willingness to take
COVID-19 vaccine booster shot
Figure 2a: Reasons for not completing the two-dose COVID-19 vaccination
Pr
ep
Figure 2b: Reasons for reluctance to receive COVID-19 vaccine booster shot
19
This preprint research paper has not been peer reviewed. Electronic copy available at: />