Tropical Neurology - part 2 pptx
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (3.4 MB, 55 trang )
44
Tropical Neurology
2
kyphus. In active disease, intraoperative traction usually results in partial correction
of the deformity. When the deformity exceeds 40˚ it may be wise to first instrument
posteriorly, achieve deformity correction and then debride and fuse anteriorly. Pos-
terior fixation is, however, not always necessary but if done helps in deformity cor-
rection and graft consolidation in the desired position. For high cervical levels, a
submandibular approach is used while the classical Southwick Robinson’s approach
suffices in other patients.
Cervicothoracic junction: Surgical options in this region are transmanubrial
anterior decompression, transclavicular anterior decompression, and high
costo-transversectomy. The transclavicular approach requires either dislocation or
surgical fracturing of the clavicle which is morbid. In addition, access to the spine is
always anterolateral and oblique. In comparison, the transmanubrial approach re-
quires splitting of only the manubrium (which is easily rejoined and heals without
nonunion), saves the thoracic duct from iatrogenic damage and, most importantly,
allows direct anterior access to the spinal column for easy grafting and fixation.
Management of Lumbosacral Tuberculosis
Backache is an important sequelae of the disease and is present in 54% of the
cases bearing a direct relation to the number of vertebrae involved and the abnormal
lumbo-sacral angles.
7
Any change in Lumbosacral angles to less than 10˚ will usually
result in accelerated degeneration and pain. Hence, surgery may be aggressively ad-
vocated in cases of acute deformity but no deficit.
Role of thoracoscopic surgery: Thoracoscopic surgery is being used for drainage of
nonresolving abscesses and for the treatment of spinal tuberculosis with paraplegia;
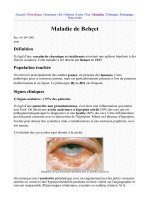
Fig. 2.11. Illustration showing the various approaches used in decompression of tuber-
culous spondylirtis.
45
Spinal Tuberculosis
2
although, its efficacy is yet to approach that of open surgery. The main advantage of
this technique lies in its minimal invasiveness and decreased morbidity.
Management of kyphosis: Radical debridement and fusion is far superior to only
debridement in adults and children past their growth sensible age. The changes in
deformity in children are similar to those in adults, although some children have a
tendency toward spontaneous correction of the deformity. Progression of deformity
in these cases is solely due to graft resorption, fracture or dislodgement with second-
ary collapse.
8
Management of Paraplegia
The general principle of management of paraplegia applies to Pott’s paraplegia
as well. Besides antitubercular and surgical therapy, general care of the paraplegic
patient is very important such as—
Bladder care: if retention—clean, intermittent self-catheterization.
Prevention of bedsores: frequent changes in position and water or air mattress.
Prevention of deep vein thrombosis: low dose heparin and physiotherapy.
Severe spasticity: baclofen, diazepam or tizanidine.
Intraspinal Tuberculous Granuloma
Intraspinal tuberculous granuloma is usually associated with Pott’s spine although
it rarely can occur without vertebral involvement. The spinal tuberculoma may be
extradural, intradural extramedullary or intramedullary.
Extradural spinal tuberculoma: Most extradural spinal tuberculomas are second-
ary to vertebral disease. A number of patients have been reported in which evi-
dences of bony tuberculosis could not be detected. These lesions are most likely due
to hematogenous spread. The patient may present with paraparesis or quadriparesis
depending on the site of the lesion. The granuloma can be visualized on spinal MRI
which can be confirmed at surgery. Treatment consists of decompressive laminec-
tomy or laminoplasty. The anterior granuloma can be safely left if decompression is
otherwise satisfactory. Antitubercular therapy is continued at least for 18 months.
Intradural spinal tuberculoma: Intradural extramedullary spinal tuberculoma is
rare and presents either as a round or oval hard mass adherent to the inner aspect of
the dura and the spinal cord or as a granulomatous mass surrounding the spinal
cord. Clinically, patients present with extramedullary compressive myelopathy.
Intramedullary spinal tuberculoma: Isolated intramedullary tuberculoma is rare.
The lesion is usually a single, hard, circumscribed mass of 7-10 mm in diameter
associated with localized arachnoiditis. The majority of these patients have associ-
ated pulmonary tuberculosis. Neurological deficit in the form of paraplegia or quad-
riplegia develops insidiously. Spinal MRI or contrast CT scan show an enhancing
lesion with or without associated perifocal edema. Intramedullary tuberculoma can
be easily enucleated under the cover of antitubercular therapy.
Tubercular Arachnoiditis
Tubercular arachnoiditis or radiculomyelopathy associated with spinal meningi-
tis refers to inflammation of the arachnoid alone or all three meninges which may
be acute or chronic, mild or severe, or localized or extensive. It is always associated
with cellular, vascular and fibrous reaction of varying degrees. Tuberculous spinal
arachnoiditis can develop in the following three ways: 1) a tuberculous lesion start-
ing primarily in the spinal meninges; 2) secondary extension from basal cranial
meningitis or 3) extension from caseous vertebra.
46
Tropical Neurology
2
The primary spinal variety of tuberculous arachnoiditis constitutes 29% of all
arachnoiditis. It is believed that spinal arachnoiditis arises as a flare-up lesion of
focal parenchymal lesion on the surface of the spinal cord similar to what happens in
cranial tubercular meningitis. The meningeal reaction varies depending on the im-
mune response of the host.
Pathology
Gross examination of the spinal cord reveals a thick collar of exudate (Fig. 2.12).
The meninges are thick, opaque and lustreless. Discrete and conglomerated tubercles
with a caseating center may be seen in the exudate. There is spinal cord atrophy. On
histopathological examination four types of changes have been reported with spinal
arachnoiditis which include borderzone rarefaction and spongification of the cord,
central necrosis, ischemic myelopathy and associated intramedullary tuberculoma.
Clinical Features
Subacute or chronic, single or multiple level and ascending or transverse
radiculomyelopathy comprise the clinical picture of spinal arachnoiditis. The sever-
ity and extent of root or cord symptoms depend on the site of maximal involve-
ment, such as a cauda equina lesion that presents as radiculopathy and higher lesions
as multifocal or single level radiculomyelopathy. No age is exempt from spinal arach-
noiditis. In the subacute form, the clinical symptoms develop on an average of two
months although maximum severity is seen within 2-5 days following, during which
time the course may be stationary. The presentation consists of root pain, paresthe-
sia, weakness, wasting and bladder dysfunction. Root pain is lancinating in charac-
ter, arising from single or multiple roots, or may be widespread. Tingling numbness
follows the root pain. Vibration and joint position sense may be impaired in the
lower limbs. Paralysis of the limbs is mostly severe and produces paraplegia or quad-
riplegia which is of upper or lower motor neuron type or a mixed variety depending
upon the extent of radiculomyelopathy. Retention of urine may be an early or a late
feature. The patient may have associated constitutional symptoms such as fever,
anorexia and weight loss.
Chronic forms of adhesive spinal arachnoiditis progress over months or years
and may be indistinguishable from spinal cord compression by a tumor. It may be
suspected if the root pain is scattered, persistent and upper motor neuron signs are
associated with lower motor neuron signs.
Investigation
CSF: There is often partial or complete subarachnoid block which may result in
a dry tap. The CSF is generally clear or xanthochromic depending on protein level
which is usually elevated. There is CSF pleocytosis ranging from a few cells to a few
hundred cells. CSF should be examined for AFB. However CSF may be normal in
localized or chronic arachnoiditis. An extra CNS source of tuberculosis should also
be explored.
Myelography: With the availability of water soluble contrast agents, myelography
is safe and commonly employed in the diagnosis of spinal arachnoiditis. The myelo-
graphic findings in spinal arachnoiditis include:
1. Slow movement of the dye column often with a filling defect and frag-
mentation of the column.
2. Total block appears as a ragged edge, or the dye column may extend ob-
liquely for two or more vertebral levels. At times there may be a pitch fork
47
Spinal Tuberculosis
2
Fig. 2.12. Dense adhesive arachnoiditis encasing the lumbar spinal cord. The transverse
section above shows exudate around the spinal cord (Courtesy Prof. S.K. Shankar).
48
Tropical Neurology
2
appearance or a distinct cut out with a concave edge of the block as seen
in spinal tumor.
3. Contrast column with or without block may show multiple small and
spotty filling defects, candle guttered appearance over a long length of
spinal cord, faggot stick or rat tail in case of cauda equina arachnoiditis
and multiple small round clear areas or a large single lesion suggesting
cyst formation.
In those in whom both cisternal and lumbar myelograms are performed, there
may be filling defect extending over many segments which have irregular columns
above and below the defect.
CT and MRI of spinal cord are preferred techniques because of the facility of the
axial section and because they are noninvasive. Spinal cord pathology is clearly seen.
CT and MRI show displacement of nerve roots of cauda equina and adherence of
roots particularly in clumps on the posterior dorsal sac. Contrast MRI reveals en-
hancement of the roots and meninges.
The final confirmation of the diagnosis is achieved by biopsy of leptomeninges.
A patient with adhesive arachnoiditis should be investigated for infective and
noninfective causes of arachnoiditis which are ennumerated in Table 2.4.
Treatment
The mainstay of the treatment of tubercular spinal arachnoiditis is antitubercu-
lar therapy on the same principles as described for tuberculous meningitis. The role
of corticosteroids is controversial. Initial oral prednisolone 1 mg/kg body weight is
given for one month and tapered over two to three months thereafter. Intrathecal
use of hydrocortisone and hyaluronidase have been reported to be useful but have
inherent risk of secondary infection. Surgery has a limited role. Surgery should be
considered if a large cyst and a localized hard band is found on imaging and its level
corresponds with clinical findings.
Summary
In tuberculosis the spinal cord can be affected in vertebral involvement, tubercu-
loma and adhesive arachnoiditis in isolation or various combinations. Spinal tuber-
culosis is the commonest form of osteoarticular disease and accounts for 50% of all
cases. Vertebral destruction, spinal deformity and paraplegia are the main attributes
of the disease. Although paradiscal disease is the commonest type, atypical presenta-
tions occur frequently in the form of extensive disease, multifocal infection, epidu-
ral granuloma, intradural abscess and posterior element disease. Diagnosis is based
on clinical features along with radiological and laboratory evidence of tubercular
infection. Despite modern imaging and laboratory techniques, tuberculous destruc-
tion at times mimics malignancy and biopsy becomes necessary for cytological and
Table 2.4. Causes of spinal adhesive arachnoiditis
Infective
Tubercular, syphilis, pyogenic, cryptococcus neoformans
Noninfective
Prolapsed intravertebral disc
Trauma
Spondylotic radiculomyelopathy
Intraspinal tumor, spinal angioma, secondaries
Drugs-Penicillin, streptomycin, anaesthetics, myodil
Idiopathic
49
Spinal Tuberculosis
2
histopathological diagnosis. In addition to eradication of the disease, prevention
and treatment of sequelae like paraplegia and deformity are the main aims of treat-
ment. Multi-drug chemotherapy is effective in the treatment of most cases of tuber-
culous spondylitis. Surgery is reserved for resistant cases, progressive deformity and
severe neurologic deficit. Paraplegia in active disease responds much better to sur-
gery than late onset paraplegia. In all cases of paraplegia, surgery must aim at ad-
equate neural recovery. In children with significant residual spinal growth,
surgery must aim at the preservation of the vertebral endplates. In this regard, a
combined anterior and posterior fusion corrects deformity and arrests its progres-
sion. The treatment of progressive kyphosis depends on the residual spinal growth,
activity of the disease and neurologic status of the patient. In general, deformity
correction is safer and easier in active than in healed disease. Implants may be used
to correct deformity and stabilize the spine.
References
1. Tandon PN, Pathak SN. Tuberculosis of central nervous system. In: Spillaine JD
ed. Tropical Neurology. London: Oxford University Press, 1973:37-62.
2. Rajasekaran, S., and Shanmugasundaram, T. K. Prediction of the angle of gibbus
deformity in tuberculosis of the spine. J Bone Joint Surg 1987; 69-A:503-509.
3. Kumar KA. Clinical classification of Posterior spinal tuberculosis. Int Orthop 1985;
9:147-152.
4. Lifeso R. Atlanto-axial tuberculosis in adults. J Bone Joint Surg 1987;
69(2):183-187.
5. Ninth Report of the Medical Research Council Working Party on Tuberculosis of
the Spine: A 10-Year Assessment of Controlled Trials of Inpatient and Outpatient
Tr eatment and of Plaster-of-Paris Jackets for Tuberculosis of the Spine in Children
on Standard Chemotherapy. Studies in Masan and Pusan, Korea. J Bone Joint
Surg 1985; 67-B (1):103-110.
6. Tuli S. Tuberculosis of the Skeletal System. New Delhi: Jaypee Brothers, 1991:268.
7. Pun WK, Chow SP, Luk KDK, Cheng CL, Hsu LCS, Leong JCY. Tuberculosis of
the lumbosacral junction. Long-term follow-up of 26 cases. J Bone Joint Surg
1990; 72-B (4):675-678.
8. Schulitz KP, John CY, Leong et al. Growth changes of solidly fused kyphotic block
after surgery for tuberculosis. Spine 1997; 22:1150-1115.
CHAPTER 3
Tropical Neurology, edited by U. K. Misra, J. Kalita and R. A. Shakir.
©2003 Landes Bioscience.
Pyogenic Infections
of the Central Nervous System
Kameshwar Prasad, Sumit Singh, Shailesh Gaekwad and Chitra Sarkar
Pyogenic infections of the nervous system include acute bacterial meningitis,
brain abscess, subdural empyema and epidural abscess. Despite the availability of
effective antibiotics, these disorders are still common and are an important cause of
morbidity and mortality. In this chapter, various pyogenic infections of the CNS are
reviewed with special reference to the tropical countries.
Acute Bacterial Meningitis
Acute bacterial meningitis (ABM) may be defined as an inflammation of the
pia-arachnoid matter and the cerebrospinal fluid (CSF) of the subarachnoid space
due to bacterial infection. The subarachnoid space extends through the brain, spinal
cord and sheaths of the optic nerves. Any infection of this space involves all the
spaces and is invariably associated with some ventriculitis.
Epidemiology
Bacterial meningitis is widely prevalent throughout the world. The incidence of
ABM is difficult to estimate, particularly in the developing countries where a large
number of patients remain unreported; however, it is probably more common in
developing than in developed countries. H. influenzae type B (Hib) is the most
important cause of meningitis in children. The majority of patients with Hib men-
ingitis are seen in the months of June to September displaying a bimodal, seasonal
variation.
1
Hib meningitis is common in children below five years of age, although
it is rare below the age of two months, probably due to transplacental transmission
of protective maternal antibodies. The occurrence of Hib meningitis is inversely
proportional to the concentration of age-related and type-specific antibodies against
the capsular antigens. Susceptibility to Hib meningitis depends upon the presence
of H. influenzae in the nasopharynx and the concentration of the type-specific
anticapsular antibodies in the host. N. meningitidis is the commonest cause of epi-
demic meningitis.
2
It has a worldwide distribution. The Sub-Saharan African region
has a ‘meningitis belt’ which extends from 5-15˚ north of the equator and includes
Chad, Dahomey, Ghana, Mali, Niger, Nigeria and Sudan. The annual incidence of
meningococcal meningitis in this endemic belt is 70/100000 population, the peak
incidence being in the months of April and May as opposed to winter and early
spring in industrialized nations. The reported cases and deaths due to meningitis in
India are summarized in Table 3.1.
Acute meningococcal meningitis is usually seen in children and young adults,
and only less than 10% cases are above 45 years of age. In the United States, the
majority of affected patients is under five years, whereas in the tropics the majority
of patients are between five and nine years.
3
Epidemics usually occur due to group A
51
Pyogenic Infections of the Central Nervous System
3
meningococcii every 8-12 year interval in the meningitis belt. This trend of the
infection is probably due to the concentration of people who do not have immunity
against the disease. For the epidemic to occur there must be enough nonimmune
individuals with the concerned pathogen. Once an epidemic occurs, the herd im-
munity of the population rises due to an increase in the nasopharyngeal carrier state.
With the passage of time, the number of nonimmune individual increases and when
a critical mass is reached, an epidemic occurs. An added factor may be a change in
the strain of the bacteria with increased virulence. The meningococcal infection
spreads through droplets from the nasopharyngeal secretions of the carriers; there-
fore, meningococcal meningitis is more common in overcrowded places such as
schools and camps.
Streptococcus pneumoniae is the commonest cause of meningitis in the adults. Its
incidence in the tropical countries is not well known. The average annual incidence
of this disease is between 1-2.3/100000 population in the United States with the
peak incidence between the months of December and May.
4
Risk factors for pneu-
mococcal meningitis are extremes of age, sickle cell disease, post-splenectomy state,
lobar pneumonia and acute otitis media. Pneumococci are the commonest cause of
recurrent meningitis following CSF leak and meningitis in acquired or primary
immunodeficiencies.
5
Etiology
The etiology of acute bacterial meningitis depends on the setting in which it
occurs. Community and hospital acquired meningitis differ widely in their bacte-
riologic spectrum.
Community Acquired Meningitis
H. influenzae, S. pneumoniae and N. meningitidis together account for about
75% of community acquired meningitis, and the remaining 25% are caused by
Gram-negative bacilli or other organisms. There is a striking age-related predisposi-
tion for different organisms to cause meningitis. The Gram-negative bacilli and the
group B streptococci are the commonest cause of meningitis in neonates, Hib and
meningococci in infants and young children, and pneumococci and Gram-negative
bacilli in adults. Gram-negative infections are common in infants and children in
developing countries. Klebsiella and Salmonella are also more common pathogens
in developing countries as opposed to the E. coli in developed countries.
6
Listeria
Table 3.1. Reported cases and deaths due to meningitis in India
Year Cases Deaths
1987 9080 1596
1988 16834 3304
1989 22263 3511
1990 16757 2984
1991 11995 2290
1992 12305 2009
1994 6496 1035
Source : Health Information India, Govt. of India (DGHS) 1994
52
Tropical Neurology
3
monocytogenes meningitis has been increasingly reported from all over the world and
is an important cause of meningitis at the extremes of age. It is more common in
alcoholics, immunocompromised individuals and patients with hematological ma-
lignancy. Patients with immunodeficiency are also more prone to Gram-negative
and pneumococcal meningitis.
Hospital Acquired Meningitis
Staphylococcus epidermidis is the commonest cause of meningitis associated
with ventriculo-peritoneal shunts at all ages. S. aureus usually causes meningitis
associated with infective endocarditis and is a common cause of post-shunt menin-
gitis, post-traumatic meningitis and infections following neurosurgical procedures.
Anaerobic bacteria account for 1% of all cases of meningitis, being under-recog-
nized, as the CSF is rarely cultured for anaerobic organisms. Chronic otitis media,
mastoiditis and sinusitis are the common predisposing conditions for anaerobic bac-
terial meningitis.
There is also a marked geographical variation in the pathogens causing meningi-
tis. Hib is the most common pathogen in the USA causing more than half of the
meningitis. In the UK, the meningococci and the pneumococci are more common
than in the USA, but the most common cause is still Hib. In the meningitis belt of
sub-Saharan Africa, the meningococcus is the most common pathogen.
Pathogenesis
The capability of an organism to cause meningitis depends on its “pathogenic
potential.” To cause meningitis, the bacteria must enter the host, colonize at a par-
ticular site, produce bacteremia and cross the blood brain barrier (BBB) to reach the
subarachnoid space where the organism easily proliferates. The infection usually
begins by colonization of the pathogen in the nasopharynx. The bacterial factors
enhancing the colonization include presence of fimbriae, which play an important
role in the adherence of meningococci to the nasopharyngeal mucosa. H. influenzae
adhere by their capsules and pneumococci by their lipopolysaccharide capsules. The
host prevents the adherence of the bacteria to the epithelium by the local secretion
of IgA. Adherence of organisms followed by activation of local immune-mechanisms
causes cytotoxicity mediated disruption of the tight junctions of the nasal epithe-
lium; loss of cilia and ciliostasis; and finally the penetration of the organisms to the
submucosa. Once the bacteria enters the submucosal bloodstream, their polysac-
charide capsules provide antiphagocytic activity. The pneumococci activate the al-
ternate complement pathway, which facilitates opsonization and subsequent
phagocytosis of the bacteria. Patients with defects in the alternative complement
pathway are at a greater risk of pneumococcal infections e.g., patients with splenec-
tomy and sickle cell disease.
The mechanism of invasion of the subarachnoid space (SAS) by the bacteria is
still under speculation. The dural venous sinuses, the thin dura over the cribriform
plate, the choroid plexus, and the monocytes have all been implicated as the site of
invasion by the organisms. The bacteria may also enter the subarachnoid space
through the hematogenous route from a parameningeal suppurative focus or through
the defects in the dura. The normal CSF has almost undetectable levels of IgM,
whereas IgG and IgA are barely detectable. The low level of complement in the CSF
accounts for the impaired opsonization and phagocytosis in patients with meningitis.
7
The meninges respond to the bacterial invasion by polymorphonuclear leukocytosis.
53
Pyogenic Infections of the Central Nervous System
3
The mechanism of entry of leukocytes into the SAS traversing the BBB is not known
although the role of a C5a complement has been suggested. In the absence of a
proper opsonic and bactericidal activity of neutrophils, there is a relentless multipli-
cation of the pathogenic organisms in the SAS resulting in inflammation of the
subarachnoid space. In meningitis, there is breakdown of the tight junctions of the
capillary endothelial cells and an increased pinocytosis across the cells. This is due to
the lipopolysaccharide capsules of the bacteria, cytokines and interleukins. The breach
of the blood brain barrier produces vasogenic cerebral edema resulting in increased
intracranial pressure (ICP) which adds to the cytotoxic and interstitial cerebral edema.
The release of toxic substances from the bacteria or neutrophils results in cytotoxic
edema and the released cells and/or molecules impair CSF flow leading to intersti-
tial cerebral edema. The inflammation of the meninges and the presence of an in-
flammatory exudate in the subarachnoid space results in vasculitis of the large blood
vessels traversing this space. This causes relative ischemia of the brain. Associated
phlebitis of the cerebral veins may result in cortical venous thrombosis or dural
sinus thrombosis which leads to focal deficits and seizures. In meningitis, cerebral
autoregulation is impaired and cerebral blood flow reduced. Recently, the role of
free radicals and reactive oxygen species in the neuronal injury in pyogenic meningi-
tis has been suggested.
Pathology
The response to bacterial invasion of the SAS is more marked over the convexi-
ties of the cerebral cortex, imparting a yellowish-green color. The exudate envelops
the basal cisterns and extends to the spinal SAS mostly to the posterior surface of the
spinal cord.
8
Microscopically, exudate shows neutrophils and bacteria in the early
stage (Fig. 3.1). As the opsonic activity of the neutrophils is impaired, live bacteria
can be demonstrated in the neutrophils. There is subintimal inflammatory infiltrate
comprising neutrophils and lymphocytes in the meningeal arteries which is unique
to pyogenic infections of the meninges. The veins also share the inflammatory re-
sponse and become distended. Mural inflammation can result in cortical venous
thrombosis with resultant cortical infarctions. By the end of the first week in un-
treated patients, the neutrophils are removed by macrophages and replaced by lym-
phocytes. Subtle changes such as edema of the subependymal and ependymal tissues,
sloughing of the ependymal lining and swelling of the astrocytes and glial cells may
be visible in the brain parenchyma. As the exudates increase, the SAS is reduced and
CSF flow may be compromised. Obstruction of the foramina of Luschka and
Magendie results in noncommunicating hydrocephalus. The inflammatory exudate
also blocks the arachnoid villi and further impedes CSF absorption, resulting in
oozing of CSF in the periventricular white matter leading to interstitial edema. The
exudate is very thick in Hib and is mostly localized to the basal cisterns, whereas it is
thinner and more extensive on the cerebral convexities in pneumococcal infections.
The SAS may be devoid of any inflammatory exudate in acute fulminant meningo-
coccemia, whereas, the interstitial edema may be very significant. These pathologi-
cal features are usually seen in the untreated cases, and the pathology is markedly
altered following antibiotic therapy.
Clinical Manifestations
Patients with ABM usually present with a classical triad of fever, headache and
altered sensorium. Almost all patients have fever and headache, but alteration in
54
Tropical Neurology
3
sensorium usually develops later. In the presence of these classical symptoms and
signs of meningeal irritation (neck rigidity and Kernig’s sign) it is easy to suspect
ABM. In adults, the classical symptoms and signs of ABM are usually evident. In a
study of 490 adult patients with ABM, fever was present in 95%, neck rigidity in
88%, seizures in 29% and alteration in sensorium 78% (6% were deeply comatose).
The most common organism isolated was S. pneumoniae.
9
Fever is of acute onset,
continuous and high grade reaching up to 38-40
0
C. Hyperpyrexia may occur, espe-
cially in the terminal phase. The pulse and respiratory rates rise with the progress of
the disease. Patients at extremes of age and in immunocompromised state may not
manifest with fever. Headache may be bifrontal but is usually diffuse, associated
with neck pain and stiffness. Vomiting is often projectile and seen with increasing
headache. Patients who present early in the course of the disease or those who are
partially treated may have a normal sensorium. A history of acute otitis media, ear
discharge, sore throat and pneumonia should be sought in all patients. Skull trauma,
CSF leak, an imunocompromised state, sickle cell anemia, diabetes, splenectomy
and long term dialysis are frequently associated with pyogenic meningitis.
Sometimes the classical features of meningitis may not be evident and a high
index of suspicion is needed. Meningitis following head trauma may be immediate
or delayed and is usually associated with CSF rhinorrhea. Such patients present with
recurrent episodes of meningitis. In these patients fever may be absent and headache
or alteration in sensorium may be the only feature. Bacterial meningitis may de-
velop after neurosurgical operations. In such patients, the pathogens are usually
Gram negative bacteria; however, the infections following ventriculo-peritoneal (VP)
shunt are usually due to staphylococci. The patients with shunt meningitis present
Fig. 3.1. Photomicrograph of a patient with pyogenic meningitis showing thickened
meninges with infiltration by inflammatory cells and congested blood vessels (H&E X
350).
55
Pyogenic Infections of the Central Nervous System
3
with fever and worsening of symptoms of raised ICP. Lumbar CSF may be normal,
therefore, CSF examination, directly from the shunt reservoir, is preferable. Dete-
rioration in sensorium may be the only indicator of ABM.
Meningitis in Children
In children the symptoms may not be typical and may manifest only with irrita-
bility and lethargy. The classical signs of neck stiffness may be absent in the early
phase of the disease. Children with meningitis have a weak, high-pitched cry, do not
respond to or stop crying on stimulation by the parents, are usually dehydrated and
appear pale. Features of raised ICP may be present in children with a fulminant
infection and include altered sensorium and poor pupillary reaction. Infants may
have bulging anterior fontanelle and older children may have papilledema. Seizures
are more common in children with meningitis compared to the adults. It is impor-
tant to differentiate children with meningitis and seizures from those with febrile
convulsions. Performing lumbar puncture in every child with febrile convulsions is
not useful in picking up extra cases of meningitis as compared to those with febrile
convulsions and signs of meningeal irritation. However, it is advisable to perform a
CSF study if the child develops meningeal signs after one to four hours of seizures,
does not show rapid recovery or if doubt of meningitis persists.
Meningitis in the Elderly
In the elderly, meningitis should be suspected if a febrile illness is associated with
altered sensorium. The fever, though present, may not be high. Alteration in senso-
rium is reported in more than 90% of patients and neck rigidity in 50%. The mor-
tality is high, being about 40%.
Diagnosis of Acute Bacterial Meningitis
The diagnosis ABM depends on clinical features and CSF analysis. Presence of
maculopopular skin rash, petechiae and hypotension due to adrenal failure
(Waterhouse-Freidrichsen’s syndrome) suggest meningococcal meningitis. A fulmi-
nant course with focal neurological deficits and subdural empyema are common in
pneumococcal meningitis. Hemophilus influenzae meningitis affects young chil-
dren and immunocompromised adults, and is commonly associated with subdural
effusion.
Lumbar Puncture and CSF Analysis
Acute bacterial meningitis results in raised intracranial pressure and may be asso-
ciated with brain abscess, subdural empyma or epidural abscess. Lumbar puncture
in the presence of raised intracranial pressure may precipitate brain herniation, which
may be fatal. However, the risk of brain herniation should be balanced against the
need to establish the diagnosis early and this decision is sometimes difficult. In
patients with fever, headache and any history of otitis media, pain in the ear, recent
head injury, facial infection, cranial osteomyelitis, focal neurologic deficit, papille-
dema and cyanotic congenital heart disease, CT scan should be carried out to
exclude space occupying lesions, but antibiotics should be administered while wait-
ing for the results of the CT scan. Before starting empirical antibiotic therapy, blood
cultures, cultures from ear, nose, throat discharges or skin rashes, if any, should be
sent. Instituting antibiotic therapy 1-2 hours before the lumbar puncture will not
decrease the diagnostic sensitivity if the culture of the CSF is done in conjunction
with testing of CSF antigens and blood culture. Samples for blood sugar should be
56
Tropical Neurology
3
withdrawn simultaneously with the CSF. The CSF is examined for cell count, pro-
tein, sugar, Gram’s stain, culture and sensitivity. The characteristic CSF findings in
pyogenic meningitis include a turbid appearance, polymorphonuclear pleocytosis,
low sugar and high protein. It is important to examine the CSF as early as possible
because the WBCs tend to disintegrate after 90 minutes. In the case of a traumatic
lumbar puncture, the correction factor for WBC count is 700 RBCs for each WBC.
If the peripheral RBC and WBC counts are deranged then the following formula
may be used.
Tr ue WBC (CSF) = Actual WBC (CSF) – WBC (Blood) x RBC (CSF)/RBC (Blood)
In a traumatic lumbar puncture, a correction of 1 mg of protein/dl should be
made for every 1000 RBC and the glucose estimation should be done as early as
possible in the supernatant after centrifugation of the CSF sample. Any delay can
lead to an erroneously low glucose report due to utilization of the glucose by the
cells. The CSF and blood glucose ratio is usually 0.6. Hyperglycemia may mask a
low CSF sugar. In the very early phase of meningitis and severe infection, the CSF
may be normocellular, but this does not exclude meningitis.
10
In such cases a repeat
CSF examination may reveal a purulent CSF after 12-24 hours. The CSF culture in
developed countries is positive in about 80% of cases, but the yield is lower in the
developing countries. Plating the CSF directly on to the culture plates improves the
positivity. Gram’s stain may be positive even if the CSF is normal. The staining can
be done from the whole CSF directly if the CSF is turbid and from the centrifuged
sediment if the CSF is clear. Acridine orange staining may be positive when Gram’s
staining is negative; it imparts a bright red color to the bacteria. However, it offers
no special advantage if the Gram’s stain is positive. In patients where Gram’s stain
and CSF culture are negative, blood culture may still be positive in 50% of the cases.
Partially treated pyogenic meningitis offers difficulties in interpretation of the CSF
reports. The Gram’s stain or culture is usually sterile after 24 hours of antibiotic
therapy. The CSF glucose rises by the third day. The CSF protein and cells are
relatively resistant and remain elevated, usually for ten days, though to a lower level.
In patients with partially treated meningitis, a negative CSF Gram’s stain and an
inconclusive CSF cytobiochemical analysis, the newer tests for rapid diagnosis, which
are described below, may be helpful.
Latex Agglutination and Counterimmunoelectrophoresis Tests
These tests depend on the demonstration of bacterial antigens in the CSF using
serum or antisera directed against the specific antigen and are sensitive and specific
for detection of Hib. Sensitivity and specificity of these tests are relatively low for
detection of other pathogens. As the tests do not require viable organisms in the
CSF, the number of false positives may be high. In 27 consecutive cases of acute
bacterial meningitis subjected to the latex agglutination test, we could detect the
antigen in only seven cases. It may be due to higher pathogenicity of bacteria in our
settings, thus causing meningitis at a lower antigenic load or our subjects may not
be mounting the level of immune response necessary for the test to be positive.
Limulus Amebocyte Lysate Test
This test can detect minimal quantities of Gram-negative pathogens and holds
some promise in meningitis following neurosurgical procedures, where Gram-negative
organisms are common. The sensitivity varies between 70% and 100%.
57
Pyogenic Infections of the Central Nervous System
3
Polymerase Chain Reaction (PCR)
PCR detects the bacterial DNA. Sensitivity and specificity of 91% has been
reported. False positives and lack of availability are the obvious limitations of PCR.
Neuroimaging
In ABM, contrast CT scan may show some enhancement of the ependyma and
the meninges. In a patient suspected of meningitis, CT scanning is indicated if the
patient has papilloedema or a focal neurological deficit to exclude a space occupying
lesion. In a patient with confirmed meningitis CT scanning is indicated if the pa-
tient develops seizures or a focal neurological deficit. Prolonged coma or fever is also
an indication for a CT scan. MRI scan can detect meningeal enhancement, focal
cerebritis, infarctions, cortical venous thrombosis and subdural effusions much bet-
ter and earlier than the CT scan, however; it is more expensive and difficult to carry
out in a semiconscious patient.
Differential Diagnosis
Viral Meningitis
In 20-25% patients with viral meningitis in the initial stage, CSF shows poly-
morphonuclear pleocytosis. Mumps, enteroviruses, herpes simplex virus and lym-
phocytic choriomeningitis reveal a low CSF glucose level. However, a repeat CSF
examination 8 to 24 hrs later shows a significant reduction of polymorphs in 90%
of patients with viral meningitis.
Brain Abscess
In a patient with ABM having focal neurologic deficit or papilloedema, brain
abscess should be considered. The CSF reveals mononuclear pleocytosis below 500/
mm
3
if abscess has not ruptured into the subarachnoid space. Contrast CT scan
usually confirms the diagnosis.
Parameningeal Infections
Subdural empyema, vertebral osteomyelitis and epidural abscess (cranial or spi-
nal) may mimic bacterial meningitis; however, CSF study reveals normal glucose
and mild mononuclear pleocytosis with mildly raised protein. Neuroimaging is helpful
in diagnosis.
Tuberculous Meningitis (TBM)
The diagnosis of TBM is relatively easy when there is a history of six weeks
duration or more and the CSF shows lymphocytic pleocytosis, raised protein and
decreased glucose. Partially treated pyogenic meningitis is difficult to distinguish
from tuberculous meningitis. A helpful point is the time between onset of the first
symptom and the onset of alteration of the sensorium. If this gap is more than one
week it favors the diagnosis of TBM, and if it is only a few days it favors pyogenic
meningitis. However, if it is between a few days to one week, extra cranial evidence
of tuberculosis or pyogenic infection should be sought; if no clue is available, it is
worthwhile to treat for both ABM and TBM. If the response is dramatic, antituber-
cular therapy should be discontinued and the patient to be kept under observation.
If the patient does not show remarkable improvement within the first few days,
antitubercular therapy is continued.
58
Tropical Neurology
3
Fungal Meningitis
Cryptococcal and candidial meningitis may also mimic bacterial meningitis and
in immunocompromised individuals may present acutely with polymorphonuclear
pleocytosis in CSF. CSF from immunocompromised individuals, therefore, should
be routinely subjected to fungal smear and culture.
Chemical Meningitis
Chemical meningitis caused by hemorrhage, spinal anesthesia, contrast media
and keratin from dermoid tumors may rarely produce a purulent CSF with a poly-
morphonuclear pleocytosis. History and CT scanning, however, resolve the issue.
Acute hemorrhagic leukoencephalitis and cerebral malaria have been reported to
produce a similar CSF profile and should be kept in mind. Unusual diseases like
SLE cerebritis, Beçhet’s syndrome and CNS angiitis may produce a similar illness
with a purulent CSF.
Complications
Cerebral Infarction
Venous or arterial infarctions may result as a consequence of thrombophlebitis
or arteritis. Focal seizures, focal deficits or increasing intracranial pressure may sig-
nal its development.
Shock
Circulatory failure may be more common in meningococcal meningitis com-
pared to other meningitis. The long-held view that adrenal failure is responsible is
no longer tenable in most cases. Much more commonly, the shock is due to a com-
bination of endotoxemia, cardiac involvement and disseminated intravascular co-
agulation.
Hydrocephalus
Communicating or obstructive hydrocephalus is seen in about 15–20% of cases.
Obstructive symptoms, delayed or in acute phase usually do not require shunting.
Subdural Effusion or Subdural Empyema
Subdural effusion is almost confined to children less than two years of age and is
reported in as high as 50% of cases. Subdural empyema, on the other hand, is very
uncommon. Both of these conditions are easily diagnosed by CT scan or MRI.
Subdural effusion is almost always self-limiting, but subdural empyema usually re-
quires craniotomy.
Cerebral Edema and Herniation
Cerebral edema and herniation may be a prominent feature in some patients
with ABM. The pathogenic effects include cytotoxic, interstitial and vasogenic edema.
The resulting raised intracranial pressure may cause cerebral herniation or reduced
cerebral blood flow.
Cranial Nerve Palsy
In ABM the third, sixth, seventh and eighth cranial nerves are commonly af-
fected. The third, sixth and seventh cranial nerves usually recover spontaneously,
but deafness is a well-known sequelae of ABM, especially in children.
59
Pyogenic Infections of the Central Nervous System
3
Treatment
Acute bacterial meningitis is a neurological emergency and is fatal if left un-
treated. Antibiotic therapy should be started immediately whenever the diagnosis is
suspected. Blood culture and CSF studies should be done as soon as possible
Choice of Antibiotics
For an antibiotic to be effective in ABM, it should be able to cross the BBB, act
in a purulent CSF and maintain a bactericidal level in the CSF long enough to kill
the bacteria. Factors which determine the level of antibiotics in the CSF are lipid
solubility, size of the molecules and protein binding. Low protein binding, small
molecular size and high lipid solubility increase the CSF availability of the drug. In
CSF the efficacy of an antibiotic depends on its metabolism. The metabolites of a
drug may or may not be as effective as the parent drugs. The concentrations of the
antibiotics in the CSF should exceed the in vitro MIC by 20-fold for optimal efficacy.
Specific Therapy for Pathogenic Bacteria
Once the reports of the culture and sensitivity are available, the antibiotics are
prescribed according to the culture reports. If culture is negative empiric therapy is
continued depending on the clinical response (Tables 3.2 and 3.3).
H. influenzae Type b (Hib) Meningitis
About one third of the strains of Hib are resistant to ampicillin, therefore a third
generation cephalosporin instead of a combination of ampicillin and chloramphemicol
is recommended by the American Academy of Pediatrics.
11
Cefotaxime and
ceftriaxone are both equally effective but the latter has the benefit of a twice-daily
regimen. Cefuroxime has been found to be less effective than cefotaxime. Gram’s
stain and CSF culture obtained after treatment with cefuroxime were found to be
positive in various trials. Cefotaxime causes an earlier sterilization of the CSF, and
has fewer complications when compared to cefuroxime for treatment of H.influenzae
meningitis.
12
Nisseria meningitidis
Strains of N. meningitidis are still sensitive to penicillin, hence, it is the drug of
choice. Partial resistance to penicillin has been reported, but still, resistance due to
production of β lactamase is extremely rare. In case of resistance or allergy to peni-
cillins, a third generation cephalosporin can be used instead.
Streptococcus pneumoniae
The incidence of drug resistance against S. pneumoniae is 20-58%. Pneumo-
cocci resistant to penicillin G at even higher MIC has been reported. Strains resis-
tant to cephalosporins have also been reported. Under such circumstances penicillin
G cannot be relied upon for the empirical treatment of pneumococcal meningitis.
In patients with mild resistance to penicillin, third generation cephalosporin should
be started and those with severe infection, a combination of vancomycin and a third
generation cephalosporin should be used. Intrathecal administration of antibiotics
is generally not required but can be considered in patients with infection due to a
highly resistant strain of pneumococcus. Newer agents like imipenem have been
used in the past, but is not used now because of it’s seizurogenic activities. Meropenem,
a carbapenem, however, is safer and holds some promise in the management of these
cases. Third generation cephalosporins (cefpirome, fluroquinolones like trovalfloxacin,
60
Tropical Neurology
3
dinafloxacin, sparfloxacin) and streptogramins e.g., (RP59500) are currently under
evaluation for pneumococcal meningitis.
13-14
Listeria monocytogenes
Ampicillin is the treatment of choice for Listeria meningitis. Patients with an
allergy to penicillin should be prescribed intravenous trimethoprim and
sulphamethoxazole in combination. Third generation cephalosporins and vanco-
mycin have not proven to be useful in the treatment of L.monocytogenes meningitis.
Gram-Negative Bacilli
Third generation cephalosporins are the drug of choice for Gram negative or-
ganisms. Traditional combinations with aminoglycosides and penicillin have a cure
rate of 40-90% as compared to the cephalosporins like ceftazidime, cefotaxime and
ceftriaxone, which cure 78-94% cases. In case of suspicion of Pseudomonas
areuoginosa, ceftazidime is preferred. Fluroquinolones like pefloxacin have been used
in patients with suspected Gram negative meningitis but should be reserved for
multi-resistant cases.
Table 3.2. Common pathogens and empiric therapeutic recommendations based
on age of patients with bacterial meningitis
Age of Patient Common Bacterial Empiric Antimicrobial
Pathogens Therapy*
1-4 weeks
Streptococcus agalactiae,
Ampicillin plus cefotaxime,
Escherichia coli, Listeria
or ampicillin plus an
monocytogenes, Klebsiella
aminoglycoside
pneumoniae, Enterococcus
species
4-12 weeks
S.agalactiae, E.coli, L.
Ampicillin plus a third
monocytogenes, H.
generation cephalosporin
influenzae, Streptococcus
pneumoniae, Neisseria
meningitislis
3 months-18 years
H. influenzae, N.
Third generation cepha-
meningitidis, S.
losporin, or ampicillin plus
pneumoniae
chloramphenicol
18-50 years
S. pneumoniae, N.
Third generation cepha-
meningitidis
losporin or benzylpenicillin*
More than 50 years
S. pneumoniae, N.
Ampicillin plus a third
meningitidis, L.
generation cephalosporin
monocytogenes,
anaerobic
Gram-negative bacilli
#Vancomycin should be added to empiric therapeutic regimens when penicillin or
cephalosporin-resistant pneumococcal meningitis is strongly suspected.
*Add ampicillin if meningitis caused by
L. monocytogenes
is suspected.
61
Pyogenic Infections of the Central Nervous System
3
Staphylococcus aureus
The drugs recommended are naficillin or oxacillin. Patients who are resistant to
these drugs usually respond to vancomycin, but the CSF penetration of vancomycin
is good in inflamed meninges only. Therefore, CSF may fail to sterilize after 48
hours. In such situation intrathecal vancomycin may be used. Tiecoplanin is emerg-
ing as a safer alternative to vancomycin with the convenience of once daily dosage
and the absence of nephrotoxicity. Rifampicin might carry an adjunctive role, which
remains to be proven.
Anaerobes
Chloramphenicol with its activity against bacteroides and penicillin with its ac-
tivity against most other anaerobes can be used for anaerobic meningitis. Metron-
idazole has excellent activity against most anaerobes and should be used with penicillin
for anaerobic meningitis.
Post-Traumatic Meningitis
With the most likely organism being pneumococcus, a third generation cepha-
losporin is the therapy of choice
Meningitis Following Neurosurgical Procedures
For procedures other than ventriculoperitoneal shunt, Gram negative organisms
are the most common pathogens. To provide cover for pseudomonas, a combina-
tion of ceftazidime with an aminoglycoside is the preferred regimen. Staphylococci
cause most post-VP shunt meningitis and should be managed with vancomycin
with or without rifampicin. Intrashunt and intraventricular vancomycin may be
tried in nonresponders.
Immunocompromised Hosts
Patients with impaired cell mediated immunity are susceptible to Listeria infec-
tion and those with impaired humoral immunity to encapsulated organisms like
pneumococus, Hib and P. aeruginosa. The treatment should include antibiotics cov-
ering both Gram positive and Gram negative bacteria, particularly pseudomonas.
Duration of Therapy
The duration of therapy depends on the suspected or isolated organism. The
patients with meningococcal and Hib meningitis usually recover with seven and ten
days therapy, respectively. Those with pneumococcus do so in two weeks. The
Gram-negative organisms need to be treated for three to six weeks. It may be noted
Table 3.3. Antibiotics dose schedule to be used in pyogenic meningitis
Penicillin G 20-24 million U/day intravenously (divided doses every 4 h)
Ampicillin 12 g/day intravenously (every 4 h)
Ceftriaxone 2-4 g/day intravenously (every 12 h)
Cefotaxime 8 g/day intravenously (every 4 h)
Ceftazidime 6 g/day intravenously (every 8 h)
Nafcillin 8-12 g/day intravenously (every 4 h)
Oxacillin 9-12 g/day intravenously (every 4 h)
Vancomycin 2 g/day intravenously (every 6 h)
62
Tropical Neurology
3
that the recommended duration of therapy is arbitrary and in individual cases it
may be prolonged if the response is unsatisfactory.
Management of Complications
Raised intracranial pressure (ICP) is a common complication of ABM. Papil-
loedema is an unreliable sign of raised ICP as it may take a few hours to days to
develop. An alteration in pupillary size, bradycardia and hypertension are signs of
impending herniation. An intracranial pressure monitoring device is useful in these
patients, and ICP above 20 mm Hg should be treated urgently and preferably treat-
ment should start as soon as the ICP is 15 mm Hg. Simple measures like head
elevation can lead to some benefit. Mannitol in a dose of 1 gm/kg given in a bolus
can reduce cerebral edema to some extent. The role of steroids in reducing cerebral
edema of bacterial meningitis is doubtful. Patients who are unresponsive to the above
medications can be helped by controlled hyperventilation or barbiturates.
Seizures
Seizures are common in children with meningitis and adults with pneumococcal
meningitis. The seizures may be due to electrolyte imbalance following poor oral
intake or a syndrome of inappropriate antidiuretic hormone (SIADH); cortical venous
thrombosis or cerebral infarction. To terminate a seizure, a short acting benzodiaz-
epine may be required followed by loading and maintenance dose of phenytoin or
phenobarbitone. Children develop SIADH sooner than adults. In adults it is man-
aged by restriction of fluids and water and by increase in sodium intake. In children,
fluid restriction can cause dehydration, particularly if fever is present. A daily re-
quirement of 1200 ml/m
2
is mandatory with 20-40 meq K
+
/m
2
body surface area.
Steroids
Corticosteroids reduce cytokine-mediated inflammation. Dexamethasone is the
most studied corticosteroid in this condition and at least 10 clinical trials have been
reported. Moreover, meta-analyses of the clinical trials suggest that dexamethasone
in children in a dose of 0.15 mg/kg body weight every six hours for four days given
just before antibiotics may be beneficial.
15-16
For adults, the benefit is doubtful.
Adjuvant Therapy
The role of nonsteroidal anti-inflammatory drugs in the therapy of experimental
meningitis has been evaluated. These drugs are associated with the prevention of
influx of leukocytes in the CSF and a reduced incidence of cerebral edema, neuro-
logical sequelae and mortality. Their clinical efficacy remains to be proven. Mono-
clonal antibodies and pentoxyphylline have also been tried as an adjunct to the
usual regimens of antibiotics without proven benefit.
Mortality
The overall mortality in ABM varies between 15-25%. It depends on a large
number of factors, namely age, duration of illness, level of consciousness, time lag
between the onset of disease and institution of therapy and the organism respon-
sible. The mortality is higher at the extremes of age. Neonates and infants have the
highest mortality. Patients with Gram negative meningitis and those with alteration
in sensorium at the time of presentation have a higher mortality.
63
Pyogenic Infections of the Central Nervous System
3
Prevention and Prophylaxis
Vaccination is the most effective means of preventing bacterial meningitis in
children. H. influenzae type b conjugate vaccine has decreased the incidence of Hib
meningitis in children in developed countries. A polyvalent vaccine containing the
polysaccharide capsule of groups A,C,Y and w 135 is currently available and is rec-
ommended for high risk children over two years of age.
Pneumococcal vaccine is derived from the capsular polysaccharide antigen from
23 serotypes of the pneumococci and is recommended only for use in high risk
children above two years of age. Conjugate vaccines against the meningococci group
A and C are currently available. The vaccine is derived from the polysaccharide
capsule of meningococci and has been responsible for the reduction of the occur-
rence of major epidemics of meningococcal group A meningitis in the developed
countries. Phase II trials with meningococcal group C vaccine have been completed,
and it holds promise for the prevention of the disease. Phase III trials are pending,
and the long term benefits of the vaccine are yet to be established.
17
Prophylaxis with rifampicin is recommended for all intimate contacts of patients
with meningococcal meningitis. Health workers in intimate contact with the in-
fected patients should also use this prophylaxis. Rifampicin is given in a dose of 10
mg/kg or a maximum of 600 mg/day for two days in children up to two years of age
and adults respectively. Alternatively, a single intramuscular injection of ceftriaxone
may be given if rifampicin is contraindicated,.as in pregnancy.
18
The household
contacts of patients with Hib meningitis should be put on a prophylactic treatment
with rifampicin, if there is at least one contact with age less than four years.
Brain Abscess
Brain abscess is defined as a focal suppurative lesion within the brain paren-
chyma. Its incidence is 0.18% to 1.3% but may be higher in developing countries.
19
Recent studies, reporting a hike in the incidence of brain abscess may be due to
availability of more sensitive diagnostic techniques. The incidence may increase be-
cause of an increased number of cases with an immunosuppressed state like AIDS
and organ transplantation. Patients undergoing neurosurgical procedures, chronic
suppurative otitis media, cyanotic congenital heart disease and infections of the
paranasal sinuses and lungs are at higher risk of brain abscess. The disease can
develop as a sequelae to pyogenic meningitis. Brain abscess is much more common
in men then in women with peak incidence at 30-45 years of age.
Etiology
The introduction of newer antibiotics has changed the spectrum of the patho-
gens causing brain abscess. Staphylococcus aureus was the most common cause of
brain abscess in the preantibiotic era but enterobacteriacae have replaced S. aureus.
Bacteroides and other anaerobes, particularly streptococci, are also important causes
of brain abscess. Patients with chronic frontal or ethmoidal sinusitis tend to have a
frontal lobe abscess and streptococcus is the most common organism. The temporal
lobe abscesses are usually associated with ear infections and are due to mixed patho-
gens. Gram negative organisms and the bacteroides are common, particularly if the
brain abscess is associated with chronic otitis media and cholesteatoma. The inter-
medius group of organisms have a striking preponderance to cause focal suppurative
lesions of the brain. Though S. pneumoniae causes bacterial meningitis frequently,
it is an uncommon cause of brain abscess except in immunocompromised states.
64
Tropical Neurology
3
Staphylococci are the most common pathogens in post-traumatic abscesses. Anaer-
obes commonly cause brain abscess and the pathogens include clostridium, bacteroi-
des and actinomycetes. The pathogenic flora for the brain abscess has changed
significantly due to an increase in the number of immumocompromised subjects
where abscesses due to Nocardia
20
are common. In immunocompromised patients
aspergillus and other dimorphic fungi are also common and account for a very high
mortality. Though cryptococcus usually causes fungal meningitis, it is known to
cause focal suppuration of the brain as well. In patients with AIDS, toxoplasma and
Entamoeba histolytica can also cause brain abscess. The prognosis in such cases is
extremely poor. The immune status of the patient can indicate the likely pathogenic
organism. Patients with T lymphocyte defects, for example AIDS patients, are mostly
affected by toxoplasma, nocardia, cryptococcus or Listeria, whereas neutropenic pa-
tients by pseudomonas or other Gram negative organisms. These patients also have
a predisposition for fungal abscess, particularly if they are on broad spectrum
antibiotics.
Pathogenesis and Pathology
The most common predisposing condition for brain abscess is ear infection.
Otogenic brain abscesses are usually located in the temporal lobes or the cerebellum.
In contrast to chronic otitis media, acute infections seldom cause brain abscesses.
Brain abscesses secondary to sinusitis are becoming increasingly rare, and the frontal
lobe is almost exclusively involved in these cases. Abscesses of dental origin are lo-
cated in the frontal or temporal lobes. Brain abscess is a rare complication of pyo-
genic meningitis except in cases of neonates with Gram negative bacterial infection.
It is uncommon to have brain abscess following trauma or brain surgery. Penetrat-
ing brain injuries and transsphenoidal pituitary surgery may result in brain abscesses.
Lung abscess and bronchiectasis are common causes of multiple brain abscesses due
to hematogenous spread, mostly in the middle cerebral artery territory. Congenital
cyanotic heart disease and infective endocarditis are other sources for hematogenous
brain abscesses accounting for 1-5% of cases.
Animal experiments have revealed that it is extremely difficult for a brain abscess
to develop in normal brain tissue. Some degree of damage to the brain is necessary
along with a source of bacteria. The spread of infection from a nearby source to the
brain tissue is either direct, through a hematogenous route or through emissary
veins, which undergo retrograde thrombophlebitis. Patients with congenital cyan-
otic heart disease are prone to cerebral microinfarctions due to polycythemia and
decreased blood flow as a result of increased viscosity of the blood. Colonization of
bacteria in these damaged areas is followed by formation of the brain abscess.
Brain abscess evolves through four stages. Early cerebritis is characterized by an
inflammatory exudate of polymorphonuclear leukocytes,which tends to localize to
the perivascular region with the development of a necrotic center. This area is sur-
rounded by cerebral edema. This state usually lasts for one to three days. Late cerebritis
usually extends from the fourth to ninth day. The necrotic center of the abscess
increases in size with neovascularization at the periphery. The capillaries are newly
formed and are surrounded by early reactive astrocytosis. There is an accumulation
of fibroblasts in the periphery which form the capsule at a later stage. Early capsule
formation extends from days 10-13. The necrotic center decreases in size and the
fibroblasts increase in number along with further neovascularization (Fig. 3.2). Late
capsule formation is the last stage after two weeks. A mature capsule is formed and
65
Pyogenic Infections of the Central Nervous System
3
with time the abscess decreases in size. The peripheral edema decreases and angio-
genesis paves way for healing (Fig.3.3).
These stages are not distinct and an alteration in this sequence is not exceptional.
The pathogens may also cause a variation in these stages according to the virulence,
such as capsule formation being poorer in organisms with high virulence, as a result
abscesses continue to increase in size and have a poorer prognosis.
Clinical Features
Fifty percent of patients with brain abscess present with a triad of fever, headache
and focal neurological deficit which is usually subacute, though a fulminant presen-
tation may rarely be seen. Focal or generalized headache of moderate to severe de-
gree is the dominant symptom. Headache may be accompanied with nausea and
vomiting. Seizures occur in 25-40% of cases, mostly in frontal lobe abscesses. Papil-
loedema and other features of raised ICP may ensue. Focal neurological deficits
occur in 50% of patients and include hemiparesis, visual field defects or cranial
nerve deficits. Patients may have varying degrees of alteration of sensorium. Neuro-
logical signs depend upon the location of the abscess, for example, temporal ab-
scesses present with aphasia, hemiparesis and field defects. The signs of associated
predisposing conditions such as ear infections, sinusitis, chest infections and con-
genital cyanotic heart disease may also be present.
Diagnosis
Lumbar puncture is contraindicated in a patient with suspected brain abscess
because of risk of herniation. The CSF picture is almost similar to pyogenic menin-
gitis; sugar is low with moderate rise of proteins and polymorphonuclear leukocytes.
In 10% of patients CSF may be normal. The CT scan with contrast enhancement
remains the radiological investigation of choice for the brain abscess. In CT scan,
abscess appears as an area of hypodensity surrounded by a uniform ring enhance-
ment and perifocal edema (Fig. 3.4-3.6). Cranial CT scan has a sensitivity of 95-99%
and a specificity of 70%. Resolving hematoma, subacute infarct, inflammatory granu-
loma and metastasis or primary neoplasia can show similar CT scan findings. The
presence of intraventricular hyperdensities and ependymal enhancement indicates
ventriculitis. MRI can provide better delineation of the brain abscess in the stage of
early cerebritis and also displays the perifocal edema better. MRI remains the inves-
tigation of choice for posterior fossa abscesses. Newer investigative modalities like
indium-III labeled leukocyte scintigraphy, 99-Tc-hexamethylpropylenamineoxime
scintigraphy and thallium-201 SPECT are currently under evaluation for the diag-
nosis of brain abscess in early stage.
Treatment
The local milieu of the abscess, the blood brain barrier and the bacterial flora of
the brain abscess, determine the response to antibiotics. The capsule of the brain
abscess impairs drug penetration, therefore, longer duration of treatment is needed.
There are no trials to support the use of a particular antibiotic regimen. Most regi-
mens include penicillin because of its excellent efficacy against streptococci. As an
alternative to penicillin, cefotaxime can be used. Due to isolation of anaerobes in
most cultures from brain abscesses, metronidazole is used. Abscesses secondary to
trauma or neurosurgical procedures should be treated with vancomycin. A common
pathogen after otitic infection is Pseudomonas aeruginosa, therefore, ceftazidime is
66
Tropical Neurology
3
Fig. 3.2. Photomicrograph of a brain abscess showing thick fibrous capsule externally
(➔) with the polymorphonuclear cell debris in the center (H & E X 350).
67
Pyogenic Infections of the Central Nervous System
3
Fig. 3.3. High powered view of a chronic abscess showing predominant infiltration by
lymphocytes and plasma cells (H & E X 750).
68
Tropical Neurology
3
included in their regimens. Only a small proportion of patients with brain abscess
respond favorably to medical treatment alone. The surgical procedures currently
used are aspiration and excision of the abscess. There are no reports of randomized
trials comparing aspiration with excision. The choice of the method depends on the
site, size, capsule thickness of the abscess as well as the choice of the surgeon. The
current consensus is that all brain abscesses should be given a trial of aspiration with
antibiotics and surgery should be reserved for larger abscesses, failed aspiration or
for posterior fossa abscess. The antibiotics should begin before surgery and continue
Fig. 3.4. Axial contrast enhanced CT scan showing a well-defined rounded lesion in the
left temporal lobe. There is peripheral ring enhancement of uniform thickness and the
central core is hypodense with perilesional edema which is suggestive of brain abscess.