Hyperopia and presbyopia - part 10 doc
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (1.58 MB, 33 trang )
296 Glazer and Azar
Table 2 Complications of LASIK for Correction of Spherical Primary Hyperopia
Mean Loss of best
No. of follow-up Technique and corrected visual
Study Year eyes (months) microkeratome used Complications acuity (BCVA)
(continued)
Suarez (25)
Ditzen (26)
Goker (27)
Knorz (28)
Esqucnazi (29)
Lindstrom (30)
1996
1998
1998
1998
1999
1999
154
43
54
23
100
46
3
12
19
12
12
6
Coherent/Schwind
Keratom II
Excimer Laser
Automated Corneal
Shaper
8.5-mm flap diameter
MEL 60 Excimer
Laser
Automated Corneal
Shaper
8.5-mm flap diameter
Keracor 116 Excimer
Laser
Automated Corneal
Shaper
8.5-mm flap diameter
Keracor 117 Excimer
Laser
Automated Corneal
Shaper
8.5-mm flap diameter
Keracor 117CT
Excimer Laser
Automated Corneal
Shaper
8.5-mm flap diameter
VISX STAR S2
Excimer Laser
Hansatome
9.5-mm flap diameter
• 1.3% corneal ectasia
• Epithelial invasion of
the interface
• Traumatic flap
displacement
• Bilateral haze
• 15% epithelial
ingrowth
• 2.3% haze
• 7.5% scars
• 4.7% vertical
decentration
• 2.3% central island
• 4.7% free cap
• 11.6% flap
dislocation
• 11.6% flap folds
• 31.4% epithelial
ingrowth
• 13%
regressed/under-
corrected
• 9.3% glare at 9
months
• 3.7% transient
diplopia that resolved
entirely
• 1.8% irregular flap
cut
• 1.8% decentration
• 3.7% irregular
astigmatism
• No significant
complications noted
• 6% epithelial
ingrowth into the
interface
• 4% scars on nasal
side
• 2% ablation
decentration
• 2% transient diplopia
• 5% flap folds
• 6.5% transient
epithelial defect
• 4.3% diffuse lamellar
keratitis
• 2% lost 1 line
• 1.3% lost 2
lines
• 9% lost 1 line
• 4.7% lost 3
lines
• 5.6% lost 2
lines
• 63% of low
hyperopes lost
1 line
• 50% of high
hyperopes lost
1 line
• 6% lost 1 line
at 1 year
follow-up
• 6% lost 2 lines
at 1 year
follow-up
• 5% lost 2 lines
at 2 year
follow-up
• 11% lost 1 line
• 2.2% lost 2
lines
297Complications of Refractive Surgery
Table 2
Continued
No. Mean Technique and Loss of best
of follow-up microkeratome corrected visual
Study Year eyes (months) used Complications acuity (BCVA)
Arbelaez (31)
Zadok (32)
Reviglio (33)
Argento (34)
El-Agha (9)
Choi (35)
1999
2000
2000
2000
2000
2001
192
72
50
147
26
32
12
6
6
12
12
6
Keracor 177C
Excimer Laser
Automated Corneal
Shaper
9.0-mm flap diameter
Nidek EC-5000
Excimer Laser
Automated Corneal
Shaper
8.5-mm flap diameter
Lasersight 200
Excimer Laser
with 9.0 software
Automated Corneal
Shaper
9.0- to 9.5-mm flap
diameter
Keracor 117C
Excimer Laser
Hansatome
5.9-mm optical zone
diameter, flap
diameter not
reported
VISX STAR S2
Excimer Laser
Hansatome
9.5-mm flap diameter
VISX S2 Smoothscan
Excimer Laser
Hansatome
9.5-mm flap diameter
• 4.3% epithelial cells
in the interface
• 2.2% haze
• 2.2% mild irreg astig
• 0.6% had a free cap
• 0.6% sterile keratitis,
(Note: Complication
rates combine the
192 spherical
hyperopes with the
164 toric hyperopes.)
• No significant
complications noted
• 2% epithelial
ingrowth in the
would edges
associated with free
caps, not requiring
surgical removal
• 8.2% transient
epithelial ulcer
• 4.5% stromal
infiltrates
• No significant
complications noted
• No significant
complications noted
• 13% of high
hyperopes lost
2 lines or more
• 1.4% lost 2
lines or more
• No eyes lost
BCVA
• Less than 5.8%
lost 1 line
• 19% lost 1 line
• 7.7% lost 2
lines
• 25% lost 1 line
• 9% lost 2 lines
a. Flap Complications
Intraoperative complications include free flaps, incomplete flaps, buttonholes, small flaps,
and thin flaps. Free flaps, thin flaps, or incomplete flaps are more likely to occur in patients
with flat (Ͻ41.00-D) and large (Ͼ11.5-mm) corneas. Unusually steep (Ͼ48.00-D) and
small (Ͻ11.5-mm) corneas are more conducive to buttonholes or large flaps.
The larger ablation areas necessary for H-LASIK require larger flaps. Extra care
must be taken with the larger flaps because a large flap may be more prone to wrinkles
298 Glazer and Azar
or misalignment, which may lead to irregular astigmatism. When pannus exists, a large
flap may cause bleeding, which must be cleared from the bed prior to ablation.
Appropriate preoperative examinations can help one identify and discourage patients
at greater risk for flap complications. Preplaced surgical landmarks that straddle the flap
edge will help with accurate repositioning of the flap in the operative and postoperative
period. In addition, the newer microkeratomes and suction rings create fewer flap complica-
tions.
b. Epithelial Ingrowth
To achieve successful H-LASIK results, the diameter of the corneal flap must be large
enough. Epithelial ingrowth can result from laser energy to the periphery of the flap, or
it may occur secondary to wound edge instability with migration of epithelial cells under
the flap (Fig. 3). Epithelial ingrowth can progress to involve the visual axis, creating
irregular astigmatism and even melting of the overlying flap (13,36).
If epithelial cells under the flap progress toward the visual axis or induce stromal
melting, the flap should be lifted, the stromal bed and flap undersurface should be thor-
oughly irrigated and scraped, and the flap should then be repositioned (37).
With larger flaps of 9 to 10 mm, the risk of epithelial ingrowth is greatly reduced,
most likely because this avoids ablation of epithelium beyond the edge of the flap (38).
Other measures one may take to prevent epithelial ingrowth include using dedicated instru-
ments exclusively for interface manipulation, so that these instruments do not come in
contact with the surrounding epithelium. Also, one should be careful to avoid flap folds,
as these may provide a conduit for cell infiltration (13).
c. Decentration
Decentration or small optical zones may lead to irregular astigmatism, causing loss of
BCVA, glare, monocular diplopia or halos, and halo effects. The same principles of de-
centration described above for PRK apply here. For example, whether with PRK or LASIK,
a larger optical zone is more forgiving of a slight decentration. More sophisticated LASIK
ablation profiles may also diminish the risk of decentration: a more gradual transition
zone between ablated and unablated tissue helps minimize epithelial and stromal regenera-
tion, with its subsequent regression.
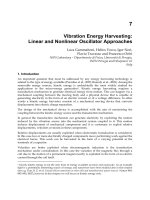
Figure 3 Epithelial ingrowth after LASIK. (A) Stable epithelial ingrowth at the LASIK interface.
(B) Retroillumination used to view the same area of epithelial ingrowth. (From Ref. 13.)
299Complications of Refractive Surgery
Figure 4 Diffuse lamellar keratitis following LASIK. (A) Diffuse lamellar keratitis 2 days after
LASIK. (B) Diffuse lamellar keratitis, 5 days after LASIK, with central coalescence, scarring, and
stromal melt. (From Ref. 13.)
d. Diffuse Lamellar Keratitis
Although diffuse lamellar keratitis (DLK) is a recently described syndrome, not yet docu-
mented after H-LASIK, it has been reported in approximately 0.2 to 3.2% of cases of
myopic LASIK (13,39–42). DLK is characterized by a proliferation of inflammatory cells
at the LASIK interface (Fig. 4). It can lead to loss of BCVA due to irregular astigmatism
and may also cause stromal corneal melting with induced hyperopia or hyperopic astigma-
tism.
The cause of DLK is still unclear; thus, prevention remains a challenge. When
present, however, DLK must be treated immediately with hourly topical prednisolone
actate 1% and broad-spectrum topical antibiotic coverage. It has been observed that if the
DLK is not resolved by the fifth postoperative day, there is typically central coalescence
of the inflammatory cells, which may lead to central stromal melting and scarring. Thus,
if inflammation progresses despite the steroid/antibiotic treatment, the flap should be lifted,
scraped, and irrigated by the fourth postoperative day at the latest (13). The use of topical
intrastromal steroid during LASIK has been proposed as a way of reducing the incidence
and severity of DLK (43).
e. Late Flap Dislocation
One rare, potential H-LASIK complication is traumatic flap dislocation, occasionally seen
months or years after LASIK (44,45). One might expect a slightly greater risk of flap
dislocation in H-LASIK because the flap tends to be wider than that created for myopic
LASIK. For this reason, it would be wise to avoid performing H-LASIK on high-risk
patients, such as boxers. One should also encourage patients to wear safety glasses when
engaging in high-risk sports activities after H-LASIK.
f. Corneal Ectasia
Corneal ectasia is a rare complication. For example, in one of the largest studies of H-
LASIK, Suarez et al. performed LASIK on 154 eyes of patients with simple hyperopia
of between ם1.00 and ם8.50 D with astigmatism of less than 0.75 D. Suarez et al. had
only two cases of postoperative corneal ectasia, both occurring in patients with high levels
of hyperopia. Keratectasia is most likely due to the mechanical uncoupling of the posterior
300 Glazer and Azar
from the anterior stroma, with subsequent weakness of the cornea. Denervation of the flap
or subclinical epithelial ingrowth may exacerbate this mechanical uncoupling. Other fac-
tors that may predispose to corneal ectasia include excessive ablation with less than 250
m of residual stromal bed, a thicker than normal flap with consequent ablation at a deeper
than planned level, and irregular corneal thickness (46). One can attempt to prevent corneal
ectasia with preoperative pachymetry maps to detect borderline cases. One must also
identify patients with keratoconus and prevent them from undergoing H-LASIK because
they, of course, would be at great risk for postoperative corneal ectasia.
g. Loss of Best Corrected Visual Acuity
Loss of BCVA is more likely to occur after H-LASIK performed on high hyperopes. Choi
notes that 50% of eyes with attempted corrections greater than5DlosttwolinesofBCVA.
These high rates of loss of BCVA in eyes with high hyperopia may be due to induced
irregular astigmatism (27–28,30–31,35). Irregular astigmatism can result from poor cen-
tration of the ablation. Even small levels of decentration can cause irregular astigmatism,
leading to degraded vision quality or monocular diplopia.
Knorz performed a pilot study on eyes with hyperopia and hyperopic astigmatism.
In eyes with ם5.1Dtoם10 D of hyperopia (15 eyes), 53% had lost one line at 1 month,
and 20% had lost two or more lines of BCVA at 1 month. For 12-month follow-up, 6
eyes were available, and 50% of these had lost one line while none had lost two or more
lines of BCVA. No significant intraoperative or postoperative complications were noted.
However, it was felt that the loss of acuity was due to image degradation by significant
optical aberrations caused by the new corneal surface. Knorz concluded his study by
suggesting that LASIK should not be used for hyperopia Ͼם5 D.(28) Studies of myopic
LASIK procedures have identified other causes of loss of BCVA to include flap folds,
epithelial defects, lamellar keratitis, and epithelial ingrowth (30).
3. Conclusion
As we gather more experience with hyperopic PRK and LASIK, we can achieve higher
rates of predictability and accuracy by creating nomograms adjusted for preoperative re-
fraction, keratometry, and age. Also, more sophisticated equipment can decrease complica-
tion rates for both PRK and LASIK: more sophisticated ablation profiles and better eye-
tracking systems can reduce decentrations. For LASIK, newer, larger microkeratomes that
produce flap diameters of at least 9.0 mm should be used.
C. COMPLICATIONS OF NONCONTACT LASER THERMAL
KERATOPLASTY
1. Background
Thermal keratoplasty (TK) was first performed in 1898 by the Dutch ophthalmologist
Lendert Jan Lans in an attempt to treat astigmatism (47). Lans demonstrated that thermal
energy, applied with a cautery, altered the structure of the corneal stromal collagen and
changed the anterior corneal curvature. Unfortunately, using simple cauteries and probes,
it was difficult to control the amount of energy applied, and TK resulted in unpredictable
results and regression (48,49). Interest in TK was rekindled with the development of lasers
that could heat the cornea in a more controlled manner.
301Complications of Refractive Surgery
Figure 5 Slit-lamp photograph of a cornea immediately after treatment with noncontact holmium:
YAG laser thermal keratoplasty. (From Ref. 55.)
In 1990, Seiler first described laser thermal keratoplasty (LTK), which utilizes the
holmium:yttrium aluminum garnet (Ho:YAG) laser to correct hyperopia (50). Ho:YAG
LTK avoids damage to the corneal epithelium by delivering infrared radiation to the mid-
stroma. LTK changes the anterior corneal curvature because corneal collagen shrinks by
30 to 45% of its original length at temperatures of 55 to 60ЊC (51). Local, peripheral
flattening causes central steepening, which corrects for hyperopia. Initially, both contact
and noncontact LTK were performed. However, contact LTK, performed by directly appla-
nating the cornea with a probe, tended to cause irregular astigmatism, regression and
undercorrection; this form of LTK was withdrawn from U.S. Food and Drug Administra-
tion (FDA) trials (52–54).
Noncontact LTK, on the other hand, has been approved by the FDA. It is traditionally
performed by projecting one to three concentric rings of eight laser spots each onto the
cornea through a slit lamp–mounted, fiberoptic delivery system (Fig. 5). FDA phase IIA
clinical trials with 2 years of follow-up showed the uncorrected visual acuity (UCVA)
was improved by one or more lines in 19 (73%) of 26 treated eyes (55).
2. Complications
While a variety of complications may occur following LTK, the most common is regression
of effect (Table 3). Short-term complications include discomfort immediately after LTK
treatment or for 1 to 3 days post-LTK; some patients complain of mild pain (18–20%),
tearing (41–43%), mild photophobia (33–41%), mild foreign-body sensation (41–54%),
and other mild discomfort (29%). These side effects of laser-induced epithelial injury
typically resolve within 3 days of treatment (56,58). Corneal opacities and epithelial haze
and staining are common in the first week post-LTK treatment. However, by 2 years after
treatment, corneal opacities at the treated sites and golden-brown intraepithelial deposits
(presumably iron deposits) in or adjacent to inferior treatment spots are typically the only
evidence of change to the cornea (56). Long-term damage to the central cornea has not
been reported as a complication.
Clearly, the principal limitation of noncontact LTK is regression. Reported rates of
regression vary from 27 to 45% (55–58). In one study, 70.1% had an UCVA of 20/20 at
302 Glazer and Azar
Table 3 Complications of Noncontact LTK for Correction of Spherical, Primary Hyperopia
Mean Loss of best
No. of follow-up Technique corrected visual
Study Year eyes (months) used Complications acuity (BCVA)
Koch (56)
Koch (55)
Alio (57)
Nano (58)
Vinciguerra (59)
1996
1997
1997
1998
1998
17
28
57
182
16
24
24
15
12
12
Sunrise
Technologies
delivery system
1 ring of 8 spots
per ring
Sunrise
Technologies
delivery system
1–2 rings of 8
spots per ring
Sunrise
Technologies
delivery system
2–3 rings of 8
spots per ring
Sunrise
Technologies
delivery system
1–3 rings of 8
spots per ring
Sunrise
Technologies
delivery system
3 rings of 8 spots
per ring
• 27% had 0.5 to 1.0
D of induced
astigmatism
• 27% regression
• 29% regression in
the 1-ring group
• 31.5% had total
regression
• 45% regression
• 0.55% decentered
treatment ring
• 0.55% with 1 D of
induced astigmatism
• 25% complained of
halos or ghost
images at 12-month
follow-up
• 6% lost 2 lines
of BCVA
• 7% lost 1 line
of spectacle-
corrected near
visual acuity
• No loss of
BCVA
• No loss of
BCVA
• No loss of
BCVA
3 months, but only 50.8% maintained this level at 15 months. In fact, by 15 months, only
57.8% were within ע1.00 D of the intended refraction (57). In addition to regression of
effect, astigmatism may occur as a result of noncontact LTK.
3. Etiology of Regression
Some researchers feel that regression is inherent to the current technique for LTK. The
Ho:YAG LTK technique delivers pulses of energy to the cornea. The pulses themselves
may trigger a mixed shrinkage/relaxation pattern. For example, if the energy pulses are
too low, an insufficient amount of collagen shrinkage is achieved, and the initial refractive
change may gradually be lost. On the other hand, if the laser heats the collagen fibrils to
65 to 70ЊC, collagen relaxation occurs.
Regression after noncontact LTK is more common in younger patients and patients
with thicker central corneas (57). Regression may be due to the elasticity of Bowman’s
membrane and stromal collagen in younger patients, which causes the cornea to return to
its previous shape. Similarly, thicker corneas may be more likely to resume their previous
configuration. At least in rabbit models, noncontact LTK provokes procollagen synthesis
by fibroblastic keratocytes, causing stromal remodeling which can produce irregularities
in the anterior corneal surface leading to epithelial hyperplasia. This in turn, results in an
303Complications of Refractive Surgery
altered corneal curvature (60). While the precise wound healing response to noncontact
LTK in humans is not known, it is possible that both regression and astigmatism may
result from a similar response.
4. Prevention
Investigators are speaking optimistically about a new continuous-wave diode laser that
can change the shape of the cornea without the peaks and troughs of the pulsed Ho:YAG
laser (61,62). The continuous-wave diode laser is expected to avoid tissue overheating,
thereby improving long-term refractive stability. In addition, FDA trials are under way
on a device that uses radiofrequency energy to the peripheral cornea; this may produce
more controlled shrinkage of collagen lamellae (63).
5. Conclusion
One point to remember is that while regression and, less frequently, astigmatism may
result from noncontact LTK, it is rare for patients to lose even one line of BCVA. No
eyes have been reported to have lost two or more lines of BCVA from noncontact LTK
(55–58). For risk-averse low hyperopes (ם0.75 to ם2.50 D), noncontact LTK is a proce-
dure to consider because it causes very few BCVA-threatening complications.
D. COMPLICATIONS OF PHAKIC INTRAOCULAR LENSES AND
CLEAR LENS EXTRACTIONS WITH INTRAOCULAR LENS
IMPLANTS
1. Background
While most types of refractive surgeries alter the cornea, the refractive power of the eye
can also be changed by implanting an intraocular lens (IOL) with or without extraction
of the crystalline lens. Barraquer implanted the first phakic intraocular lens in the 1950s
(64). Unfortunately, many of these anterior chamber lenses were poorly finished and had
sharp edges. After Barraquer had implanted almost 500 lenses, significant complications
such as corneal edema occurred, and over 300 of the lenses had to be removed (65). After
this experience, interest in phakic IOLs waned until labs were better able to guarantee the
quality of IOLs.
Intraocular lenses being made today are of much better quality than those used in
the 1950s. A recent study used a scanning electron microscope to analyze the surface
quality of new-generation phakic IOLs; the study showed that these lenses did not have
any defects that would contraindicate their use as phakic IOLs (66). This study examined
the three major types of lenses currently used as phakic IOLs: anterior chamber lenses
(currently used only in myopic eyes), iris-fixated anterior chamber lenses, and posterior
chamber lenses.
2. Complications
Even when perfectly constructed IOLs with smooth surfaces are placed, there is still a
risk of progressive corneal endothelial cell loss secondary to phakic IOLs (67–71). Other
304 Glazer and Azar
Table 4
Complications of Phakic Intraocular Lens Implantation for Correction of Hyperopia
Mean Loss of best
No. of follow-up IOL corrected visual
Study Year eyes (months) Implanted Complications acuity (BCVA)
Davidorf (76)
Rosen (77)
Fechner (78)
Pesando (79)
Sanders (80)
Pershin (81)
1998
1998
1998
1999
1999
2000
24
9
69
15
10
33
18
6
120
18
6
12
Staar ICL
Staar ICL
Iris-Claw IOL
Staar ICL
Staar ICL
Storz Phacoprofile
IOL
• 12.5% pupillary
block glaucoma
• 8% IOL
decentration of
more than 1 mm
• 12.5% underwent
removal of their
IOL
• 11% pupillary block
glaucoma, requiring
surgical iridectomy
and removal of IOL
• 1.4% lens
dislocation
secondary to
postoperative
trauma
• 3% uveitis, corneal
edema, and
glaucoma
• 13% pupillary block
glaucoma
• 6.7% anterior
• No complications
• 6% anterior
subcapsular cataract
• 3% lens
replacement was
required due to
calculation error
• 9% pigment
dispersion without
IOP elevation
• 4% lost 3
lines
• 22% lost 1
line
• No loss of
BCVA
• 6.7% lost
2 lines
• No loss of
BCVA
• No loss of
BCVA
potential complications of IOL implantation include cataract formation, pupillary-block
glaucoma, endophthalmitis, and retinal detachments (Table 4) (72–75).
Currently the most popular phakic IOL for the treatment of hyperopia is the Collamer
Staar Posterior Chamber IOL, also called the implantable contact lens (ICL) (Fig. 6). A
recent phase I trial of silicone plate posterior chamber lenses, implanted in hyperopes,
reported that 100% of patients had 20/40 or better UCVA, and 70% had 20/20 or better
UCVA (80).
In one study of hyperopes with phakic IOLs 1 year after implantation, opacities in
the area of lens contact with the capsule developed in two eyes (6%). Pigment dispersion
occurred in three eyes (9%), but without intraocular pressure elevation. One eye (3%)
required a lens replacement because of a calculation error (81). Another study reported
305Complications of Refractive Surgery
Figure 6 The STAAR Collamer posterior chamber phakic intraocular lens implant. (From Ref.
79.)
an anterior subcapsular cataract developing immediately after surgery in one eye (6.7%),
causing a loss of two lines of BCVA (79).
Because hyperopic eyes tend to be shorter, they are more prone to pupillary block
after implantation of posterior chamber lenses. One study using the Staar Collamer Im-
plantable Contact Lens (ICL) reported 2 of 15 eyes (13%) developing a severe pupillary
block despite two iridotomies that had been performed 2 weeks prior to surgery. The
increased intraocular pressures due to the pupillary block necessitated removal of the
implants (79). Another study of the Staar ICL reported a 12.5% incidence of postoperative
pupillary block. In addition, IOL decentration of more than 1 mm occurred in 2 of the 24
eyes (76).
Sight-threatening complications such as endophthalmitis have been reported to occur
in phakic IOL procedures for myopia and could theoretically occur for hyperopic phakic
IOL implantation procedures as well (75). Occasionally, silicone plate phakic intraocular
lenses need to be removed due to incorrect sizing of the lens and poor fixation within the
sulcus (82). Retinal detachments after phakic IOL implantation have been reported in
4.8% of myopic eyes (74). This complication has not yet been reported in hyperopic eyes.
Iris-fixated phakic IOLs for the correction of high hyperopia can be associated with
serious complications such as corneal decompensation and glaucoma (Fig. 7) (78). Other
risks include cataract formation and glaucoma (pupillary block glaucoma, pigmentary
glaucoma, narrow-angle glaucoma, and malignant glaucoma) (76). Peripheral iridotomies
can treat or prevent pupillary-block glaucoma. Shallow anterior chambers should be a
contraindication to performing an ICL because of the risk of narrow-angle glaucoma. Lens
decentration may also occur.
3. Clear Lens Extraction with IOL Implantation
Clear lens extraction (CLE) with IOL placement has been studied as a surgical correction
of hyperopia. Some of the disadvantages associated with this procedure as a treatment for
myopia are not as a relevant when it is considered as a hyperopic treatment. For example,
306 Glazer and Azar
Figure 7 The Fechner iris-claw intraocular lens implant. (From Ref. 78.)
myopes are more prone to retinal detachments (RDs). But the increased risk of an RD
after clear lens extraction surgery is less relevant in hyperopes. In addition, the loss of
accomodation that accompanies removal of the crystalline lens is a moot point in the high
hyperope, who can see neither at distance nor at near without correction. One problem of
CLE with IOL placement encountered with hyperopes, which is not relevant in myopes, is
the potential need to implant more than one IOL (piggyback IOLs) to correct for hyperopia.
Several recent studies on clear lens extraction for hyperopia demonstrate that this
is a safe and effective procedure. Kolahdouz-Isfahani performed clear lens extraction on
18 eyes. Two eyes lost two lines of BCVA, but no reason for the loss of BCVA was
found after a complete ocular examination was performed. Complications included one
case of postcapsular opacification requiring one YAG capsulotomy, one case of a lens
dislocation requiring an IOL exchange, and one case of malignant glaucoma (83). Another
study of 35 eyes reported that no eyes lost BCVA postoperatively. Additional procedures
consisted of one IOL exchange and one PRK for overcorrection, both due to IOL miscalcu-
lations. Posterior capsular opacification developed in 19 eyes (54.2%), requiring 19 YAG
capsulotomies (84). One study of 20 eyes that underwent clear lens extraction and IOL
implantation reported no complications; there was no loss of BCVA and no need for
further procedures. The authors did find, however, that the procedure was less accurate
and less predictable for less than ם3.00 D of hyperopia (85).
Pop et al. performed CLE with IOLs followed by PRK or LASIK. The only post-
CLE complication in this study was interlenticular opacification (ILO), which occurred
in 14 eyes that had piggyback polyacrylic lenses. Of the initial 65 eyes in the study, 40
eyes received two IOLs (piggyback IOLs) because the lens power needed was higher than
30 D. Thus, 35% of all the piggybacks developed interlenticular opacification. There were
no other reported complications from the CLE surgery (86).
307Complications of Refractive Surgery
Other potential risks of clear lens extraction surgery with IOL implants include the
risks associated with any cataract surgery, such as hemorrhage, retinal detachment, cystoid
macular edema, and endophthalmitis. Approximately 10% of high hyperopes have axial
lengths of less than 21 mm, predisposing them to choroidal effusions.
4. Prevention
As with any type of surgery, many surgical complications of phakic IOL surgery or CLE/
IOL surgery decrease with surgeon experience. Visual complications such as halo and
glare are significantly reduced with increased optic size from 5.0 to 6.0 mm.
When iris-claw lenses are used, the risk of corneal decompensation can be decreased
by using adequate viscoelastic during surgery, so that the IOL does not touch the cornea;
ensuring sufficient anterior chamber depth; and providing long-term monitoring of the
corneal endothelium (78).
Glaucoma is always a potential problem associated with IOL implantation in small,
hyperopic eyes. During clear lens extraction with IOL implantation, peripheral iridectomies
should be performed in eyes with corneal diameters of 11.0 mm or less or axial lengths
of 20 mm or less. Peripheral iridotomies should be performed prior to the implantation
of phakic IOLs.
5. Conclusion
While many daunting complications may occur secondary to phakic IOL implantation or
CLE/IOL implantation, there are certainly many advantages to treatment of hyperopia
with either of these techniques. First, IOL implantation is the only refractive procedure
that can correct higher degrees of hyperopia. Second, it uses skills that physicians who
perform cataract surgery have honed and polished. Finally, it does not require expensive
equipment, such as lasers. Hopefully, more long-term data will be available in the future
to help decrease the rate of potential complications associated with phakic IOL surgery.
E. COMPLICATIONS OF INTRACORNEAL SEGMENTS AND LENSES
1. Background
Intacs, the intrastromal corneal ring segment (ICRS), consists of two 160-degree poly-
methyl methacrylate (PMMA) segments placed in two pockets of the peripheral stroma
(Fig. 8). The procedure is unique in that it retains the potential to be adjusted or reversed.
Figure 8 The Intrastromal corneal ring. (From Ref. 91.)
308 Glazer and Azar
In April 1999, the FDA approved Intacs for myopic correction of מ1.00 to מ3.00
D with ם1.00 D or less of astigmatism. Intacs can also be used to create central corneal
steepening to correct for hyperopia. Studies are currently investigating the use of small
linear segments placed in the peripheral cornea to create shortening of the peripheral length
of the corneal arc, with subsequent central corneal steepening. By altering the thickness
of the insert, one can titrate the refractive effect.
Although there have been no published studies on Intacs for hyperopia, clinical trials
are currently under way in Germany and Spain. These trials have produced promising
preliminary results: study ࠻1 enrolled 19 patients, and at 1 year 95% (18 of 19) achieved
an UCVA of 20/40 or better. Of note, an induced astigmatism of 1.00 D or greater was
seen in 32% (6 of 19) of the cases. Eleven patients were enrolled in study ࠻2, with 6
months of follow-up. Ten of the 11 eyes (91%) were 20/40 or better, and 4 eyes (36%)
experienced an induced astigmatism of 1.00 D or more. Finally, study ࠻3 enrolled 9
patients with 6 months follow up. All patients had an UCVA of 20/40 or better; only 1
patient had an induced astigmatism equal to or greater than 1.00 D (87).
2. Complications
Published studies of Intacs today are for the correction of myopia. However, the complica-
tions of Intacs would be similar whether the segments were placed for the correction of
myopia or for hyperopia. In the FDA phase II and III studies, the incidence of adverse
events was 2% of the 452 eyes enrolled. Complications of the ICRS procedure include
accidental perforation into the anterior chamber (2 eyes), surface perforation of the epithe-
lium anteriorly (3 eyes), significant decentration of the rings requiring removal or reposi-
tioning (5 eyes), and infectious keratitis (1 eye). All eyes in the group of patients with
complications returned to preoperative BCVA by their 6-month follow-up appointment
(88).
Schanzlin reported no serious complications in the 125 eyes that received ICRS in
his study. Minor postoperative problems included one case of transient conjunctivitis,
three cases of filamentary keratitis, and one case of transient iritis. One patient, whose
incision had gone into a region of superior pannus, developed deep stromal blood vessels.
At 12 months follow-up, four patients had a two-line loss of BCVA, from 20/12.5 to 20/
20. All four of these patients had a substantial improvement in their UCVA (89).
Postoperative astigmatism is clearly a significant potential problem, with 20 of 102
patients in one group experiencing post-ICR astigmatism of 1.0 D or more at 3 months
follow-up. Various theories exist as to the cause of the astigmatism; it may be related to
suture tightness (90). Induced astigmatism may also result from postoperative movement
of the intracorneal ring segments. Finally, Intacs-induced astigmatism can result from
irregular stromal and epithelial thickening between the Intacs rings (91).
Reports describe one patient with persistent focal edema due to a small Descemet’s
tear from a lamellar dissection that was too deep. Although the edema necessitated ICR
removal, the patient’s BCVA was 20/20 at exit from the study. One of 102 patients incurred
an intraoperative perforation of Descemet’s membrane, requiring an ICRS explantation
(90). Channel deposits associated with Intacs are occasionally seen but are not associated
with impaired visual acuity (88,89).
3. Prevention
One can attempt to prevent postimplant complications through meticulous attention to
positioning, proper incision depth and pocketing, and sterile technique. In addition, proper
309Complications of Refractive Surgery
attention to wound architecture along with adequate closure and tissue approximation with
suturing can minimize the frequency of wound-related complications such as wound gape
and epithelial cysts. One can prevent corneal neovascularization status post-ICRS by avoid-
ing incisions that make contact with pannus or a limbal blood vessel and by warning
against eye rubbing so as to prevent wound dehiscence.
4. Conclusion
Intacs may prove to be a valuable tool for the correction of hyperopia. Advantages over
procedures such as LASIK and PRK include the fact that the Intacs insert is placed in the
peripheral cornea and the central cornea is never violated during the surgical procedure.
In addition, the Intacs devices can easily be removed if necessary. Finally, the refractive
effect can be adjusted by replacement of any of the implanted radial segments. The compli-
cation of induced astigmatism may become less of an issue as more Intacs devices are
implanted: the cause of induced astigmatism may become better understood and thus better
prevented. In addition, surgical technique will be improved as more of these surgeries are
performed.
F. CONCLUSION
Clearly, since hyperopic refractive surgery is entirely elective, the surgeon must have a
thorough understanding of any potential complications of each type of procedure. The
risk/benefit balance is tipping in favor of H-PRK, H-LASIK, or noncontact LTK for low
to moderate hyperopes and toward intraocular lens implantation with or without clear lens
extraction for moderate to high hyperopes. The use of ICRS for hyperopia may be useful
for low to moderate hyperopes; however, long-term results of current studies have yet to
be reported.
Thorough preoperative evaluations and preventive techniques such as those de-
scribed above can help to avoid complications. However, even with the most prepared
surgeon and in the best of hands, complications may occur. Thus, it is essential to provide
patients with a clear understanding of the potential risks of a procedure before proceeding.
REFERENCES
1. Sorsby A. Biology of the eyes as an optical system. In: Duane TD, Jaeger EA, eds. Clinical
Ophthalmology. Philadelphia: Lippincott, 1988:1394–1414.
2. Leibowitz HM, Krueger DE, Maunder LR, Milton RC, Kini MM, Kahn HA, Nickerson RJ,
Pool J, Colton TL, Ganley JP, Loewenstein JI, Dawber TR. The Framingham Eye Study
Monograph. VIII. Visual acuity. Surv Ophthalmol 1980; 24(suppl):472–479.
3. Daya SM, Tappouni FR, Habib NE. Photorefractive keratectomy for hyperopia: six-month
results in 45 eyes. Ophthalmology 1997; 104:1952–1958.
4. Jackson WB, Casson E, Hodge WG, Mintsioulis G, Agapitos PJ. Laser vision correction for
low hyperopia. An 18-month assessment of safety and efficacy. Ophthalmology 1998; 105:
1727–1738.
5. Williams DK. One year results of laser vision correction for low to moderate hyperopia.
Ophthalmology 2000; 107:72–75.
6. Marshall J, Trokel S, Rothery S, Schubert H. An ultrastructural study of corneal incisions
induced by an excimer laser at 193 nm. Ophthalmology 1985; 92:749–758.
310 Glazer and Azar
7. Marshall J, Trokel S, Rothery S, Krueger RR. Long-term healing of the central cornea after
photorefractive keratectomy using an excimer laser. Ophthalmology 1988; 95:1411–1421.
8. Isfahani AH, Pangilinan R, Shah S. Surgical correction of hyperopia. Ophthalmol Clin North
Am 1997; 9(part 4):599–615.
9. El-Agha MSH, Johnston EW, Bowman RW, Cavanagh HD, McCulley JP. Excimer laser
treatment of spherical hyperopia: PRK or LASIK? Trans Am Ophthalmol Soc. 2000; 98:
59–65.
10. Haw WW, Manch EE. Prospective study of photorefractive keratectomy for hyperopia using
an axicon lens and erodible mask. J Refract Surg 2000; 16:724–730.
11. Pacella E, Abdolrahimzadeh S, Balacco Gabrieli C. Excimer laser photorefractive keratectomy
for hyperopia. Ophthalm Surg Lasers 2001; 32:30–34.
12. O’Brart DP, Stephenson CG, Oliver K, Marshall J. Excimer laser photorefractive keratectomy
for the correction of hyperopia using an erodible mask and axicon system. Ophthalmology
1997; 104:1959–1970.
13. Melki SA, Azar DT. LASIK complications: etiology, management, and prevention. Surv Oph-
thalmol 2001; 46:95–116.
14. Gartry DS, Kerr-Muir MG, Lohmann CP, Marshall J. The effect of topical corticosteroids on
refractive outcome and corneal haze after photorefractive keratectomy. Arch Ophthalmol 1992;
110:944–952.
15. O’Brart DP, Lohmann CP, Klonos G, Corbett MC, Pollock WS, Kerr-Muir MG, Marshall J.
The effects of topical corticosteroids and plasmin inhibitors on refractive outcome, haze and
visual performance after excimer laser photorefractive keratectomy: a prospective, randomised,
observer-masked study. Ophthalmology 1994; 101:1565X74.
16. Gartry DS, Kerr Muir MG, Marshall J. The effect of topical corticosteroids on refraction and
corneal haze following excimer laser treatment of myopia: an update. A prospective, random-
ized, double-masked study. Eye 1993; 7:584–590.
17. Fagerholm P, Hamberg-Nystrom H, Tengroth B, Epstein D. Effect of postoperative steroids
on the refractive outcome of photorefractive keratectomy for myopia with the Summit excimer
laser. J Cataract Refract Surg 1994; 20(suppl):212–215.
18. Stojanovic A, Nitter TA. Correlation between ultraviolet radiation level and the incidence of
late-onset corneal haze after photorefractive keratectomy. J Cataract Refract Surg 2001; 27(3):
404–410.
19. Corbett MC, O’Brart DP, Warburton FG, Marshall J. Biologic and environmental risk factors
for regression after photorefractive keratectomy. Ophthalmology 1996; 103:1381–1391.
20. Siganos DS, Katsanevaki VJ, Pallikaris IG. Correlation of subepithelial haze and refractive
regression 1 month after photorefractive keratectomy for myopia. J Refract Surg 1999;
158–342.
21. Xu H, Shuangzhen L, Xia A, Huang P, Wang P, Wu X. Mitomycin C reduces haze formation
in rabbits after excimer laser photorefractive keratectomy. J Refract Surg 2001; 17:342–349.
22. Majmudar PA, Forstot SL, Dennis RF, Nirankari VS, Damiano RE, Brenart R, Epstein RJ.
Topical mitomycin-C for subepithelial fibrosis after refractive corneal surgery. Ophthalmology
2000; 107(1):89–94.
23. Ojeimi G, Waked N. Laser in situ keratomileusis for hyperopia. J Cataract Refract Surg 1997;
13(suppl):432–433.
24. Sinan G, Hamdi E, Cegmi K. Laser in situ keratomileusis to correct Hyperopia from ם4.25
to ם8.00 diopters. J Cataract Refract Surg 1998; 14:105.
25. Suarez E, Torres F, Duplessie M. LASIK for correction of hyperopia and hyperopia with
astigmatism. Int Ophthalmol Clin 1996; 36(4):65–72.
26. Ditzen K, Huschka H, Pieger S. Laser in situ keratomileusis for hyperopia. J Cataract Refract
Surg 1998; 24:43–47.
27. Goker S, Er H, Kahvecioglu C. Laser in situ keratomileusis to correct hyperopia from ם4.25
to ם8.00 diopters. J Refract Surg 1998; 14:26–30.
311Complications of Refractive Surgery
28. Knorz MC, Liermann A, Jendritza B, Hugger P. LASIK for hyperopia and hyperopic astigma-
tism—results of a pilot study. Semin Ophthalmol 1998; 13(2):83–87.
29. Esquenazi S, Mendoza A. Two year follow-up of last in situ keratomileusis for hyperopia. J
Refract Surg 1999; 15:648–652.
30. Lindstrom RL, Hardten DR, Houtman DM, Witte B, Preschel N, Chu YR, Samuelson TW,
Linebarger EJ. Six-month results of hyperopic and astigmatic LASIK in eyes with primary
and secondary hyperopia. Trans Am Ophthalmol Soc 1999; 97:241–260.
31. Arbelaez MC, Knorz MC. Laser in situ keratomileusis for hyperopia and hyperopic astigma-
tism. J Refract Surg 1999; 15:406–414.
32. Zadok D, Maskaleris G, Montes M, Shah S, Garcia V, Chayet A. Hyperopic laser in situ
keratomileusis with the Nidek EC–5000 excimer laser. Ophthalmology 2000; 107(6):
1132–1137.
33. Reviglio VE, Bossana EL, Luna JD, Muino JC, Juarez CP. Laser in situ keratomileusis for
myopia and hyperopia using the Lasersight 200 laser in 300 consecutive eyes. J Refract Surg
2000; 16(6):716–723.
34. Argento CJ, Cosentino MJ. Comparison of optical zones in hyperopic laser in situ keratomi-
leusis: 5.9 mm versus smaller optical zones. J Cataract Refract Surg 2000; 26(8):1137–1146.
35. Choi RY, Wilson SE. Hyperopic laser in situ keratomileusis: primary and secondary treatments
are safe and effective. Cornea 2001; 20(4):388–393.
36. Castillo A, Diaz-Valle D, Gutierrez AR, Toledano N, Romero F. Peripheral melt of flap after
laser in situ keratomileusis. J Refract Surg 1998; 14:61–63.
37. Walker MB, Wilson SE. Incidence and prevention of epithelial growth within the interface
after laser in situ keratomileusis. Cornea 2000; 19:170–173.
38. O’Brart DP. The status of hyperopic laser in situ keratomileusis. Curr Opin Ophthalmol 1999;
10:247–252.
39. Lin RT, Maloney RK. Flap complications associated with lamellar refractive surgery. Am J
Ophthalmol 1999; 127:129–136.
40. Linebarger EJ, Hardten DR, Lindstrom RL. Diffuse lamellar keratitis: diagnosis and manage-
ment. J Cataract Refract Surg 2000; 26:1072–1077.
41. Smith RJ, Maloney RK. Diffuse lamellar keratitis. A new syndrome in lamellar refractive
surgery. Ophthalmology 1998; 105:1721–1726.
42. Stulting RD, Carr JD, Thompson KP, Waring III GO, Wiley WM, Walker JG. Complications
of laser in situ keratomileusis for the correction of myopia. Ophthalmology 1999; 106:13–20.
43. Peters NT, Lingua RW, Kim CH. Topical intrastromal steroid during laser in situ keratomileusis
to retard interface keratitis. J Cataract Refract Surg 1999; 25:1437–1440.
44. Lemley HL, Chodosh J, Wold TC, Bogie CP, Hawkins TC. Partial dislocation of laser in situ
keratomileusis flap by air bag injury. J Refract Surg 2000; 16:373–374.
45. Geggel HS, Coday MP. Late-onset traumatic laser in situ keratomileusis flap dehiscence. Am
J Ophthalmol 2001; 131(4):505–506.
46. Vinciguerra P, Camesasca FI. Prevention of corneal ectasia in laser in situ keratomileusis. J
Refract Surg 2001; 17(suppl):S187–S189.
47. Lans LJ. Experimentelle Untersuchungen uber Entstehung von Astigmatismus durch nichtperf-
oririende Corneawunden. Arch Ophthalmol 1898; 45:117–152.
48. Stringer H, Parr J. Shrinkage temperature of eye collagen. Nature 1964; 204:1307.
49. Neumann AC, Sanders D, Raanan M, DeLuca M. Hyperopic thermokeratoplasty: clinical
evaluation. J Cataract Refract Surg 1991; 17:830–838.
50. Seiler T, Matallana M, Bende T. Laser thermokeratoplasty by means of a pulsed holmium:
YAG laser for hyperopic correction. Refract Corneal Surg 1990; 6:335–339.
51. Allain JC, Lous LE, Cohen-Solal: Isometric tensions developed during the hydrothermal swell-
ing of rat skin. Connect Tissue Res 1980; 7:127–133.
52. Durrie DS, Schumer DJ, Cavanough TB. Holmium:YAG laser thermokeratoplasty for hyper-
opia. J Refract Corneal Surg 1994; 10:S277–S280.
312 Glazer and Azar
53. Goggin M, Lavery F. Holmium laser thermokeratoplasty for reversal of hyperopia after myopic
photorefractive keratectomy. Br J Ophthalmol 1997; 81:541–543.
54. Tutton MK, Cherry PKM. Holmium:YAG laser thermokeratoplasty to correct hyperopia: two
years follow-up. Ophthalmic Surg Lasers 1996; 27(5 suppl):S521–S524.
55. Koch DD, Kohnen T, McDonnell PJ, Menefee R, Berry M. Hyperopia correction by noncontact
holmium:YAG laser thermal keratoplasty: U.S. Phase IIA clinical study with 2-year follow-
up. Ophthalmology 1997; 104:1938–1947.
56. Koch DD, Abarca A, Villarreal R, Menefee R, Kohnen T, Vassiliadids A, Berry M. Hyperopia
correction by noncontact holmium:YAG laser thermal keratoplasty: clinical study with 2-year
follow-up. Ophthalmology 1996; 103:731–740.
57. Alio JL, Ismail MM, Sanchez Pego JL. Correction of hyperopia with non-contact Ho: AG
laser thermal keratoplasty. J Refract Surg 1997; 13:17–22.
58. Nano HD, Muzzin S. Noncontact holmium:YAG laser thermal keratoplasty for hyperopia. J
Cataract Refract Surg 1998; 24:751–757.
59. Vinciguerra P, Kohnen T, Azzolini M, Radice P, Epstein D, Koch DD. Radial and staggered
treatment patterns to correct hyperopia using noncontact holmium:YAG laser thermal kera-
toplasty. J Cataract Refract Surg 1998; 24:21–30.
60. Koch DD, Kohnen T, Anderson JA, Binder PS, Moore MN, Menefee RF, Valderamma GL,
Berry MJ. Histologic changes and wound healing response following 10-pulse noncontact
holmium:YAG laser thermal keratoplasty. J Refract Surg 1996; 12:623–634.
61. Bende T, Jean B, Oltrup T. Laser thermal keratoplasty using a continuous wave diode laser.
J Refract Surg 1999; 15:154–158.
62. Geerling G, Koop N, Brinkman R, Tungler A, Wirbelauer C, Birngruber R, Laqua H. Continu-
ous-wave diode laser thermal keratoplasty: first clinical experience in blind human eyes. J
Cataract Refract Surg 1999; 25:32–40.
63. Sher NA. Hyperopic refractive surgery. Curr Opin Ophthalmol 2001; 12:304–308.
64. Barraquer J. Anterior chamber plastic lenses. Results of and conclusions from five years of
experience. Trans Ophthalmol Soc UK 1959; 79:393–424.
65. Drews RC. The Barraquer experience with intraocular lenses, 20 years later. Ophthalmology
1982; 89:386–393.
66. Kohnen T, Baumeister M, Magdowski G. Scanning electron microscopic characteristics of
phakic intraocular lenses. Ophthalmology 2000; 107:934–939.
67. Landesz M, Worst JGR, van Rij G. Long-term results of correction of high myopia with an
iris claw phakic intraocular lens. J Refract Surg 2000; 16:310–316.
68. Mimouni F, Colin J, Koffi V, Bonnet P. Damage to the corneal endothelium from anterior
chamber intraocular lenses in phakic myopic eyes. Refract Corneal Surg 1991; 7:277–281.
69. Saragoussi JJ, Cotinat J, Renard G, Savoldelli M, Abenhaim A, Pouliquen Y. Damage to the
corneal endothelium by minus power anterior chamber intraocular lenses. Refract Corneal
Surg 1991; 7:282–285.
70. Perez-Santonja JJ, Iradier MT, Sanz-Iglesias L, Serrano JM, Zato MA. Endothelial changes
in phakic eyes with anterior chamber intraocular lenses to correct high myopia. J Cataract
Refract Surg 1996; 22:1017–1022.
71. Menezo JL, Cisneros AL, Rodriguez-Salvador V. Endothelial study of iris-claw phakic lens:
four-year follow-up. J Cataract Refract Surg 1998; 24:1039–1049.
72. Trindade F, Pereira F. Cataract formation after posterior chamber phakic intraocular lens
implantation. J Cataract Refract Surg 1998; 24:1661–1663.
73. Brauweiler PH, Wehler T, Busin M. High incidence of cataract formation after implantation
of a silicone posterior chamber lens in phakic, highly myopic eyes. Ophthalmology 1999; 106:
1651–1655.
74. Ruiz-Moreno JM, Alio JL, Perez-Santonja JJ, de la Hoz F. Retinal detachment in phakic eyes
with anterior chamber intraocular lenses to correct severe myopia. Am J Ophthalmol 1999;
127:270–275.
313Complications of Refractive Surgery
75. Perez-Santonja JJ, Ruiz-Moreno JM, de la Hoz F, Giner-Gorriti C, Alio JL. Endophthalmitis
after phakic intraocular lens implantation to correct high myopia. J Cataract Refract Surg 1999;
25:1295–1298.
76. Davidorf JM, Zaldivar R, Oscherow S. Posterior chamber phakic intraocular lens for hyperopia
of ם4toם11 diopters. J Refract Surg 1998; 14:3.
77. Rosen E, Gore C. Staar Collamer posterior chamber phakic intraocular lens to correct myopia
and hyperopia. J Cataract Refract Surg 1998; 24:596–606.
78. Fechner PU, Singh D, Wulff K. Iris-Claw lens in phakic eyes to correct hyperopia: preliminary
study. J Cataract Refract Surg 1998; 24:48.
79. Pesando PM, Ghiringhello MP, Tagliavacche P. Posterior chamber collamer phakic intraocular
lens for myopia and hyperopia. J Refract Surg 1999; 15:415–423.
80. Sanders DR, Martin RG, Brown DC, Shepherd J, Deitz MR, De Luca M. Posterior chamber
phakic intraocular lens for hyperopia. J Refract Surg 1999; 15:309–315.
81. Pershin KB, Pashinova NF. Refractive Surgery of Hyperopia. J Refract Surg 2000; 16(suppl):
S242-S246.
82. Zaldivar R, Oscherow S, Giselle R. The STAAR Posterior Chamber Phakic Intraocular Lens.
Int Ophthalmol Clin 2000; 40:237–244.
83. Visessook N, Peng Q, Apple DJ, Gerl R, Schmickler S, Schoderbek RJ Jr, Guindi A. Pathologi-
cal examination of an explanted phakic posterior chamber intraocular lens. J Cataract Refract
Surg 1999; 25:216–222.
84. Kolahdouz-Isfahani AH, Rostamian K, Wallace D, Salz JJ. Clear lens extraction with intraocu-
lar lens implantation for hyperopia. J Cataract Refract Surg 1999; 15(3):316–323.
85. Siganos DS, Pallikaris IG. Clear lensectomy and intraocular lens implantation for hyperopia
from ם7toם14 diopters. J Cataract Refract Surg 1998; 14:105–113.
86. Lyle WA, Jin GJ. Clear lens extraction to correct hyperopia. J Cataract Refract Surg 1997;
23(7):1051–1056.
87. Pop M, Payette Y, Amyot M. Clear lens extraction with intraocular lens followed by photore-
fractive keratectomy or laser in situ keratomileusis. Ophthalmology 2001; 108(1):104–111.
88. Verity SM. Intacs for myopia and hyperopia. Refractive Surgery 2001, American Academy
of Ophthalmology Annual Meeting, New Orleans, 2001, pp 83–87.
89. Linebarger EJ, Song D, Ruckhofer J, Schanzlin DJ. Intacs: the Intrastromal Corneal Ring. Int
Ophthalmol Clin 2000; 40:199–208.
90. Schanzlin DJ. Studies of Intrastromal Corneal Ring Segments for the correction of low to
moderate myopic refractive errors. Trans Am Ophthalmol Soc 1999; 97:815–890.
91. Burris TE. Intrastromal corneal ring technology: results and indications. Curr Opin Ophthalmol
1998; 9:9–14.
92. Reinstein DZ, Srivannaboon S, Holland SP. Epithelial and stromal changes induced by Intacs
examined by three-dimensional very high frequency digital ultrasound. J Refract Surg 2001;
17:310–318.
28
Future Developments
BRIAN S. BOXER WACHLER
Boxer Wachler Vision Institute, Beverly Hills, California, U.S.A.
Presently, there are several viable treatments for the correction of hyperopia and presby-
opia. In order to broaden the scope of patient acceptance, current and investigative tech-
niques will continue to develop in the future as the clinicians and researchers strive for
greater efficacy, safety, and visual quality. Each area within refractive surgery will bring
improvements specific unto itself.
A. HYPEROPIA
1. LASIK and PRK
Hyperopic laser-assisted in situ keratomileusis (LASIK) and photorefractive keratectomy
(PRK) have the advantage of directly reshaping the cornea with high safety in low to
moderate degrees of correction. There is growing interest in where hyperopic ablations
should be centered on the eye. Conventional teaching is to center treatments on the pupil-
lary center. This paradigm has developed from a 1987 article by Uozoto and Guyton
(1)
that demonstrated, through mathematical analysis, the rationale for pupil centration of
refractive procedures. An opposing article by Pande and Hillman
(2)
used another set of
analyses to show that the corneal sighted light reflex (which best approximates the visual
axis of the eye) is the best location for centering refractive procedures. Positive angle
kappa (corneal sighted light reflex located nasal to pupilary center) is not nearly as common
in myopes as it is in hyperopes
(3)
. Therefore, since the excimer was used initially for
myopia, the potential for decentered ablations due to pupilary centration was low. I believe
that the combination of delayed hyperopic excimer capability and the lower number of
such patients undergoing treatments has obscured the issue that hyperopic ablations and
perhaps myopic ablations as well may be better centered on the corneal sighted light reflex.
Over 2 years ago, I began to question the recommendation of the Uozoto and Guyton
315
316 Boxer Wachler
Figure 1 Decentration of the treatment zone is seen in the right eye compared to the left eye in
the hyperopic patient will bilateral angle kappa. The laser ablation was centered on the pupil in the
right eye and on the coaxially sighted corneal light reflex in the left eye.
article after noting the decentrations of hyperopic LASIK was not uncommon in my
practice. In one hyperopic patient with angle kappa, I centered the hyperopic treatment
on the pupil on the first eye; on the second eye, the treatment was centered on the corneal
sighted light reflex
(4)
. The postoperative topographies demonstrate decentration of the
treatment in the eye where the laser was centered on the pupil, while the fellow eye showed
a centered ablation (Fig. 1). This area will undergo further study, evaluating not only
topography but also visual acuity, contrast sensitivity, and higher-order aberrations.
The dioptric limits of hyperopic excimer correction are not entirely clear. Therefore,
there will be better definitions of the limitations of hyperopic ablations, which may be
defined by acceptable degrees of induced higher-order aberrations. The pupil is the guard-
ian of the aberrations of the eye. Based on individual pupil-dependent aberrations, future
studies will likely determine the limits of hyperopic treatments.
In myopic LASIK, the flap itself has been shown to be a source of higher-order
aberrations, specifically spherical aberrations
(5)
. In hyperopic LASIK, it is unknown what
role flap-induced aberrations play. We can expect to see such evaluations in the future
for hyperopic LASIK compared to hyperopic PRK.
2. Thermokeratoplasty
Laser thermokeratoplasty (LTK)has the advantage of being very safe due to its noncontact
modality, which also avoids surgery in the central cornea. As an indirectly acting proce-
dure, one of its limitation is that the variable corneal steepening may occur with the same
317Future Developments
degree of treatment, also that some eyes have more instability of the effect than others.
The future of LTK lies in the ability to perform intraoperative, real-time refractive monitor-
ing using wavefront analysis during the treatment. This may allow the surgeon to stop
the treatment when the desired refractive effect is achieved, making the treatment indepen-
dent of corneal physiology, dehydration, stiffness, and surgeon technique. Preliminary
results of lower-energy treatments hold promise for more stable postoperative effects.
Like LTK, conductive keratoplasty (CK) offer the advantage of avoiding the central
cornea. CK will be evaluated for additional uses, as for astigmatism, by steepening the
flat axis (opposite to astigmatic keratotomy, whereby the steep axis is flattened). The
ability of the probe to be used selectively may make this device useful for treating irregular
astigmatism, as in keratoconus. Focal heat treatments of keratoconus have been evaluated
in the past, but the controlled temperature gradient of CK may lead to more stability than
previous probe technologies.
3. Intraocular Lenses
Phakic intraocular lenses offer the advantage of high-quality of vision in higher corrections
as well as being removable. Phakic lenses will continue to undergo safety evaluation with
longer-term follow-up. Such lenses have the ability to treat higher degrees of hyperopia
than excimer lasers. Wavefront analysis will help determine the optical advantages of
phakic implants compared to excimer laser treatments. Adjustability of lens power may
be achieved in the future through exchangeable optic with a haptic carrier or thoroughly
laser adjustments of the optic postimplantation.
B. PRESBYOPIA
1. Scleral Expanding Bands
Scleral expansion surgery, although not without controversy, has been slowly gaining
credibility. The data from international and preliminary U.S. Food and Drug Administra-
tion clinical trial results demonstrate improved reading ability postoperatively. As a result,
there will be greater attention paid to refining this technique and improving accommodative
predictability. Ultrasound will be used to elucidate the relationship to segment positioning
relative to zonules and lens capsule and how this affects postoperative accommodative
amplitudes. Surgical intrumentation will improve, thus decreasing the duration of what is
now an approximately 45-min procedure. The new device, called the “Focal One,” is an
automated blade that creates the belt loops and has already improved efficiency in perform-
ing the procedure.
2. Multifocal LASIK and Intraocular Lenses
Presbyopic LASIK has the advantage of improving near vision in carefully selected pa-
tients. Wavefront analysis will be an important adjunct to help elucidate the acceptable
induced aberrations that maximize near vision without compromising quality of vision.
Some monofocal intraocular lenses made with wavefront optic profiles have been reported
to improve near vision with distance as well. Accomodating endocapsular intraocular
lenses will continue to be evaluated for longer-term safety and efficacy.
318 Boxer Wachler
C. Conclusions
We are beginning a new era as refractive surgery now embraces the challenge of correcting
presbyopia. Through the creativity and determination of many ophthalmic care providers
and investigators, greater numbers of patients are experiencing the increased freedom that
comes with treating hyperopia and presbyopia. The future is very bright for the surgical
correction of hyperopia and presbyopia.
References
1. Uuzoto H, Guyton DL. Centering corneal surgical procedures. Am J Ophthalmol 1987; 103:
264–275.
2. Pande M, Hillman JS. Optical zone centration in keratorefractive surgery. Entrance pupil center,
visual axis, coaxially sighted corneal reflex, or geometric corneal center? Ophthalmology 1993;
100:1230–1237.
3. Burian HM. The sensorial retinal relationships in comitant strabismus. Arch Ophthalmol 1947;
37:336–340.
4. Korn T, Chandra N, Boxer Wachler BS. Visual outcomes of hyperopic LASIK: centration based
on pupil center versus visual axis. American Society of Cataract and Refractive Surgery Annual
Meeting, April 2001.
5. Roberts C. Flap-induced spherical aberrations. Videorefractiva Italy Ophthalmology Congress.
February 2001.
Accommodative mechanism, debate, 34
Accommodative tone, 211
Accommodative triad, 31
ACS (See Anterior ciliary sclerotomy (ACS))
ACS-SEP, 214
Age-related cataract (ARC), 58
Aging
crystalline lens, 55–63
size and shape, 56–57
oxidative stress, 58–59
presbyopia, 57–58
refractive error, 57
zonule, 60
AIS, 223–224, 232
ALK, 5, 164
Alternating-vision bifocal contact lenses, 68
American Optical vectographic test, 195
Ametropia
correctable modeling, 272
correction, 261
simultaneous within Phaco-Ersatz, 269
AMO ARRAY, 238, 239
foldable silicone multifocal intraocular
lens, 250
Amplitude of accommodation, 19
simultaneous ametropia correction
Phaco-Ersatz, 263–264
Index
Aberrations
defined, 151
hyperopia vs. myopia, 159
Ablation zone decentration, 294
Accommodating and adjustable intraocular
lens (IOL), 279–285
results, 283–284
Accommodation
defined, 30–31
Fincham, 40–42
Gullstrand, 39–40
Helmholtz description, 32–33
measurement, 36–38
near vision, 19–20
optical changes, 30–32
scleral expansion surgery, 44
Accommodative amplitude, 20, 213
after surgery for presbyopia, 287–290
dynamic retinoscopy, 287–288
increased depth of focus, 289
measuring accommodation, 289–290
multifocal crystalline lens, 289
retinoscopic reflexes, 288–289
wavefront analysis, 290
Accommodative apparatus, anatomy, 27–28
Accommodative intraocular lens (IOL)
finite-element computer simulation, 10
319
Anesthesia, hyperopic phakic intraocular
lenses, 122
Anisometropic blur-suppression test, 195
Anterior chamber phakic intraocular lens
hyperopia, 115–117
contraindications, 116
indications, 116
optic folding, 116
preoperative management, 117
visual outcomes, 117
Anterior ciliary sclerotomy (ACS), 9–10,
211, 212–214
enhanced, 213
future directions, 216
interocular pressure, 215–216
Anterior ciliary sclerotomy with implantation
of scleral expansion plugs (ACS-
SEP), 214
Anterior ischemic syndrome (AIS), 223–224,
232
Antibiotics, hyperopic phakic intraocular
lenses, 124
Aphakic epikaratophakia, 130
Apoptosis, keratocytes, 174–176
ARC, 58
Array implantation, 251
Array lens, 251
Array multifocal intraocular lens in situ, 254
Artisan hyperopia, 6
Artisan hyperopia lens, 119–120, 121
Artisan iris-claw lens, 125
hyperopic phakic intraocular lenses,
122–125
Artisan phakic intraocular lens (IOL)
hyperopia, 124
Astigmatism, 67, 159, 178
hyperopic, 80–82
cross-cylinder technique, 80–82
treatment, 82
irregular, 136
rigid gas permeable lens, 67
thermal keratoplasty, 164
Automated lamellar keratoplasty (ALK), 5,
164
Axis variation, 82
Badal optical system, 52
Baikoff foldable contact lenses, 6
Barraquer cryolathe, 4
Beaver Dam Eye Study, 23
Best spectacle-corrected visual acuity
(BSCVA), 110
Bifocal contact lens, presbyopia, 9, 68
320 Index
Bifocal spectacle, first, 134
Binocular depth of focus, 196–197
Binocular inhibition, 196
Binocular summation, 196
Binocular visual acuity, 196
Blur circles, 247
BMP, 174
Bone morphogenic proteins (BMP), 174
Brucke’s muscle, 28
BSCVA, 110
Calibrated marker, 227
Capsulorhexis, 254
Carbon dioxide laser, 84
Cataracts
age-related, 58
oxidative stress, 58–59
presbyopia multifocal IOLs, 240–241
refractive surgery, 237
Central corneal power, 136–137
Chromatic aberrations, 152–153
Ciliary muscle, 28–29, 35
magnetic resonance imaging, 51
CK (See Conductive keratoplasty (CK))
CK Keratoplast tip, 96
Clear lens extraction (CLE), with IOL
placement, 305–307
Cobalt magnesium fluoride laser, 164
Coma pattern, 155
Compound cylindrical hyperopic errors,
correction, 145–146
Computed videokeratography (CVK), 129
Conductive keratoplasty (CK), 133–134
device, 97
examinations, 98
hyperopia, 7, 95–105
thermokeratoplasty procedures, 95–96
mechanism, 96–97
patient selection, 97–98
performing, 98–100
postoperative care, 100
procedure, 97–98
radiofrequency-based, 96
for reducing hyperopia, 255
United States multicenter clinical trial,
100–105
corneal topography, 102
efficacy, 101
patients and methods, 100
results, 101–105
safety, 104–105
slit lamp, 104
stability, 103