- Trang chủ >>
- Y - Dược >>
- Gây mê hồi sức
THỞ MÁY CHO BỆNH NHÂN NONARDS
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (9.9 MB, 37 trang )
CHƯƠNG TRÌNH ĐÀO TẠO Y KHOA LIÊN TỤC
THỞ MÁY CHO BỆNH NHÂN
NON-ARDS
Trình bày: BSCK1. Nguyễn Lý Minh Duy
TP. HCM, ngày 17 tháng 12 năm 2019
TỔNG QUAN
• 1543 Vesalius, concept of mechanical
ventilation
• 1774 Joseph Priestly and Willhelm
Scheele independently discovered
oxygen
à mouth to mouth resuscitation by Tossach
DISCOVERIES SERIES
ATS DISCOVERIESATS
SERIES
ventilation is a life-sustaining
Mechanical ventilation is a Mechanical
life-sustaining
the treatment of patients with
therapy for the treatment oftherapy
patientsforwith
acute respiratory failure. It isacute
a veryrespiratory
common failure. It is a very common
modality
in intensive care units, and indeed
modality in intensive care units,
and indeed
the the
advent
the advent of its use heralded
dawnofofits use heralded the dawn of
care units. Interest in
modern intensive care units.modern
Interestintensive
in
mechanical ventilation has mechanical
increased ventilation has increased
markedly
from both a research and a clinical
markedly from both a research
and a clinical
perspective over the past 15perspective
years sinceover
the the past 15 years since the
publication
publication of a milestone article
in theof a milestone article in the
New England
New England Journal of Medicine
by the Journal of Medicine by the
investigators
that highlighted the
ARDSNet investigators thatARDSNet
highlighted
the
importance
of a lung-protective ventilation
importance of a lung-protective
ventilation
strategy (1).
strategy (1).
Although recognition of theAlthough recognition of the
importance
importance of lung protection
appears toofbelung protection appears to be
relatively
new, there are fascinating accounts
relatively new, there are fascinating
accounts
dating
dating back hundreds of years
thatback
link hundreds of years that link
ventilation
ventilation to the development
of lung to the development of lung
injury.
In this
injury. In this article, I provide
a very
brief,article, I provide a very brief,
relatively
personal perspective of the history
relatively personal perspective
of the history
of mechanical
of mechanical ventilation, with
an emphasisventilation, with an emphasis
Figure 1. (Left) Woodcut of theFigure
only known
firsthand
likeness
Andreas
(reprinted
1. (Left)
Woodcut
of theofonly
knownVesalius
firsthand
likeness of Andreas Vesalius (reprinted
on ventilator-induced lung on
injury
(VILI).
ventilator-induced
lung injury (VILI).
from Reference 48). (Right) Frontispiece
of De Humani
Corporis
Fabricaof(reprinted
fromCorporis Fabrica (reprinted from
from Reference
48). (Right)
Frontispiece
De Humani
I focus on historical aspectsI of
bothon historical
focus
aspects 49).
of both
Reference
Reference 49).
TỔNG QUAN
1900s-1950: Negative ventilation
• 1864: Alfred Jones first body enclosing
device
• 1929: Drinker and Shaw The first iron lung
ATS DISCOVERIES SERIES
Figure 4. Pneumatic chamber: Patented by Wilhelm Schwake in Germany in 1926 (51). Schwake
was concerned with precise matching of the ventilator and the patient’s breathing pattern. Reprinted
from Reference 13.
understanding of ventilator-induced
diaphragmatic dysfunction (19).
Many of these improvements have
clearly led to much better ventilators and
discussed a previous publication by William
Tossach. Tossach had helped resuscitate
a coalminer who was apneic and pulseless.
“Tossach had applied his mouth close to
the patient’s and by blowing strongly,
holding the nostrils at the same time, raised
his chest fully by his breath. The surgeon
felt 6–7 quick beats of the heart . . . . In one
hour the patient began to come to himself,
within four hours, he walked home, and
in as many days returned to his work” (11).
Later on in the Discussion Fothergill
writes “It has been suggested to me by some
that a pair of bellows might possibly be
applied with more advantage in these cases,
than the blast of a man’s mouth; but if any
person can be got to try the charitable
experiment by blowing, it would seem
preferable to the other [because] the lungs
of one man may bear, without injury, as
great a force as those of another man can
exert; which by the bellows cannot always
be determined” (11). Fothergill clearly
understood the possibility of injury caused
by ventilation and in many ways can be
viewed as the father of VILI, with his
incredibly insightful conclusions 270 years ago.
In 1829, d’Etioles demonstrated that
using bellows for ventilation could cause
pneumothoraces, leading to death. This
study was widely interpreted as suggesting
that the lungs of a patient who was
pulseless could not tolerate positive
pressure ventilation. This likely set the field
back many years. Indeed, in 1837 the Royal
Humane Society removed the use of
bellows as well as mouth-to-mouth
resuscitation from its list of recommended
treatments (20).
Mechanical ventilation was originally
introduced in patients with normal lung
function, essentially to replace the
neuromuscular pump (e.g., comatose
TỔNG QUAN
1950 to the present
• Bjorn Ibsen & Lassen : positive airway
pressure ”hand bagged” à mortality of polio
patients 87 % to 40 %
• Revolution of ventilator: flow delivery
exhalation valves, microprocessors, triggering,
flow delivery, and the development of new
modes of ventilation
• Barach & Ashbaugh: positive end-expiratory
pressure (PEEP)
TỔNG QUAN
BAROTRAUMA
VOLUTRAUMA
“Air leaks”
Volume not
PIP
Injurious
Mediators and
Mechanotransduction
Systemic
inflammation
Role for
PMNs
00
90
19
80
19
70
19
19
1
Early ICUs
Genomics/
Proteomics
Diffuse
lung
injury
60
Ventilation
and surfactant
B
E
D
S
I
D
E
BIOTRAUMA
20
B
E
N
C
H
ATS DISCOVERIES SERIE
“Baby lung”
of
ARDS
Respirator
lung
Surfactant
trials
YIE LD
3
1 positive
3 negative
vent. trials
Large
positive
vent.
trial
Yield normal
blood gas to
low V strategy
gure 7. Timeline highlighting a number of basic science (top) and clinical (bottom) observations that have had an impact on our current understan
TỔNG QUAN
TỔNG QUAN
• Thơng khí cơ học cứu mạng (?) à
Gây tổn hại
• ARDS
– Thơng khí giảm Vt tăng PEEP/ ARDS
– High Driving Pressure à VILI
• Non – ARDS ?
– Low Vt
– High PEEP
– Low Driving Pressure
LOW TIDAL VOLUME
PROS
Tác giả
Thiết kế
So sánh
Kết cục
Lee
1990
RCT
103 BN
12 vs 6
ml/kg
Vt thấp ít biến chứng hơ
hấp, thời gian thở máy ngắn
Gajic O
2005
RCT
3261 BN
10 vs 6
ml/kg
Nguy cơ ARDS tăng gấp 5
lần
Determann
2010
RCT
150 BN
10 vs 6
ml/kg
Vt thấp ít bị ARDS hơn
Serpa Neto
2015
Cohort
2184 BN
>10 vs <7
ml/kg
Nguy cơ biến chứng hô hấp
OR 0,72 (0,52 ; 0,98)
7 – 10 ml/kg Không khác biệt
Sjoding MW
2019
Cohort 1905 > 8ml/kg
Tăng tỷ lệ tử vong
OR12 1,66 (1,15 - 2,38)
OR24 1,51 ( 1,08 - 2,11)
CARING FOR THE
CRITICALLY ILL PATIENT
LOW TIDAL VOLUME
CARING FOR THE
CRITICALLY ILL PATIENT
Association Between
Association Between Use of Lung-Protective Ventilation With Low
Ventilation With Lower
Tidal Volumes
PROTECTIVE VENTILATION AND LOWERand
TIDALClinical
VOLUMES Outcom
and Clinical Outcomes Among Patients
Without Acute Respir
Acute Respiratory Distress Syndrome A Meta-analysis
, Without
0.10Table 2. Demographic, Ventilation, and Laboratory Characteristics of the Patients at the Final
A Meta-analysis
mL/kg
Ary Serpa Neto, MD, MSc
Follow-up Visit
Se´rgio Oliveira Cardoso, MD
the
de- Neto, MD, MSc
Ary Serpa
Context Lung-protective mechanical ventilation withMean
the use of(SD)
lower tidal volumes
has been found to improve outcomes of patients with acute respiratory distress syn- Jose´ Antoˆnio Manetta, MD
Se
´ rgio OliveiraĐIỂM
Cardoso, MD DÂN
ĐẶC
SỐ
convendrome (ARDS). It has been suggested that use of lower tidal volumes also benefits Victor Galva˜o Moura Pereira, MD
Jose´ Antoˆnio Manetta, MD
Conventional
patients who do not have ARDS. Protective
nlyVictor
ranDaniel Crepaldi Espo´sito, MD
Galva˜o Moura Pereira, MD
P
Ventilation
Objective To determine whetherVentilation
use of lower tidal volumes is associated
with imManoela de Oliveira Prado
proved outcomes of patients receiving
Crepaldi Espo´sito, MD
asDaniel
0.26
Value
(n ventilation
= 1416)who do not have ARDS.(n = 1406)
Pasqualucci, MD
Data Sources MEDLINE, CINAHL, Web of Science, and Cochrane Central Register
Manoela de Oliveira Prado
. Pasqualucci, MDAge, y
Maria Cecı´lia Toledo
59.97 (7.92)
60.22 (7.36)
.93
of Controlled Trials up to August 2012.
Maria Cecı´lia Toledo
Weight, kg
Damasceno, MD, PhD
Tidal
Marcus J. Schultz,
MD,volume,
PhD
M
Damasceno, MD, PhD
Study Selection Eligible studies evaluated
use of lower vs higher tidal volumes
in pa72.71 (12.34)
72.13
(12.16)
.93
tients without ARDS at onset of mechanical ventilation and reported lung injury devel- Marcus J. Schultz, MD, PhD
a
mortality, pulmonary6.45
infection,
atelectasis, and biochemical10.60
alterations.
(1.09)
(1.14)
Ͻ.001
mL/kgopment,
IBW overall
M
ECHANICAL VENTILATION
Data Extraction Three reviewers extracted data on study characteristics, methods,
is a life-saving
in pa- ECHANICAL
6.40 by
(2.39)
3.41 (2.79)
.01 strategy
PEEP, cm
H2O a and outcomes. Disagreement was resolved
VENTILATION
consensus.
in patients with acute
a life-saving strategy Data Synthesis
Twenty articles (2822
participants)
using
respiratory failure.
pressure, cm H2O a
16.63
(2.58)were included. Meta-analysis
21.35
(3.61)
.006 Howtilation isinPlateau
patients with acute a fixed-effects
model showed a decrease in lung injury development (risk ratio [RR], 0.33; ever, unequivocal evidence suggests
respiratory
failure.rate,
How- 95% CI, 0.23 to 0.47; I , 0%; number
needed
to treat [NNT], 11), and mortality
Respiratory
18.02
(4.14)
13.20(RR,
(4.43)
.01 has the
9; NNT,
that mechanical ventilation
ever, unequivocal evidence suggests
0.64; 95% CI, 0.46 to 0.89; I , 0%; NNT, 23) in patients receiving ventilation with lower
a
breaths/min
potential
to
aggravate
and
precipitate
that inmechanical ventilation has the tidal volumes. The results of lung injury development were similar when stratified by
nary
In
acute
respiratory
dislung
injury.
a,b of study (randomized vs nonrandomized)
the type
and were significant only in9.13
randompotential to aggravate
and precipitateL/min
8.46 (2.90)
(2.70)
.72and in a
Minute-volume,
tress
syndrome
(ARDS),
nition)
lung injury. In acute respiratory dis- ized trials for pulmonary infection and only in nonrandomized trials for mortality. Metamilder form of ARDS formerly
showed,
in protective ventilation groups,
a lower
Pa(ARDS),
O2/FIO2 aand in a analysis using a random-effects model
304.41
(65.74)
312.97
(68.13)
.51 known
tress syndrome
incidence of pulmonary infection (RR, 0.45; 95% CI, 0.22 to 0.92; I , 32%; NNT, 26), as acute lung injury (ALI), mechanie group
milder form of ARDS formerly known
stay (6.91
[2.36] vs 8.87 [2.93] days, respectively;
PaCO(ALI),
Hg a lower mean (SD) hospital length of41.05
(3.79)
37.90 (4.19)
cal ventilation can cause.003
ventilator2, mm
mechanias acute
lung injury
wer
V
standardized mean difference [SMD], 0.51; 95% CI, 0.20 to 0.82; I , 75%), higher mean associated lung injury. VentilatorT
a
cal ventilationpH
can cause ventilator- (SD) PaCO levels (41.05 [3.79] vs 37.90 [4.19]
mm Hg, respectively; SMD, −0.51;
95%
(0.03)
7.40
(0.03)
associated lung injury is.11
a frequent
CI,associated
0.22 lung injury. Ventilator- CI, −0.70 to −0.32; I , 54%), and lower7.37
mean (SD) pH values (7.37 [0.03] vs 7.40 [0.04],
complication
in
critically
ill
patients
Abbreviations:
F
IO
,
fraction
of
inspired
oxygen;
IBW,
ideal
body
weight;
PEEP,
positive
end-expiratory
pressure.
injury is a frequent respectively; SMD, 1.16; 95% CI, 0.31 to 2.02; I , 96%) but similar mean (SD) ratios of
2;associated
95% lungina Atcritically
O to fraction of inspired oxygen (304.40 [65.7] vs 312.97 [68.13], respectively; SMD, receiving mechanical ventilation, and
the final
visit.
complication
ill follow-up
patients Pa
2
2
1
1
2
2
2
2
2
2
2
b
2
2
2
Context Lu
has been foun
drome (ARDS
patients who
Objective T
proved outco
Data Source
of Controlled
Study Selec
tients without
opment, over
Data Extrac
and outcome
Data Synthe
a fixed-effects
95% CI, 0.23
0.64; 95% CI,
tidal volumes
the type of stu
ized trials for p
analysis using
incidence of p
lower mean (S
standardized m
(SD) PaCO2 lev
CI, −0.70 to −
respectively; S
PaO2 to fractio
0.11; 95% CI
did not influe
CARING FOR THE
CRITICALLY ILL PATIENT
CARING FOR THE
CRITICALLY ILL PATIENT
LOW TIDAL VOLUME
Association Between
Association Between Use of Lung-Protective Ventilation With Low
Ventilation With Lower Tidal Volumes
and Clinical Outcom
and Clinical Outcomes Among Patients
Without Acute Respir
Without Acute Respiratory Distress Syndrome A Meta-analysis
A Meta-analysis
Ary Serpa Neto, MD, MSc
Se´rgio Oliveira Cardoso, MD
Jose´ Antoˆnio Manetta, MD
Victor Galva˜o Moura Pereira, MD
Daniel Crepaldi Espo´sito, MD
Manoela de Oliveira Prado
Pasqualucci, MD
Maria Cecı´lia Toledo
Damasceno, MD, PhD
Marcus J. Schultz, MD, PhD
KẾT CỤC
Ary Serpa Neto, MD, MSc
Se´rgio Oliveira Cardoso, MD
Context Lung-protective mechanical ventilation with the use of lower tidal volumes
has been found to improve outcomes of patients with acute respiratory distress syn- Jose´ Antoˆnio Manetta, MD
drome (ARDS). It has been suggested that use of lower tidal volumes also benefits Victor Galva˜o Moura Pereira, MD
patients who do not have ARDS.
Daniel Crepaldi Espo´sito, MD
Objective To determine whether use of lower tidal volumes is associated with imManoela de Oliveira Prado
proved outcomes of patients receiving ventilation who do not have ARDS.
Pasqualucci, MD
Data Sources MEDLINE, CINAHL, Web of Science, and Cochrane Central Register
Maria Cecı´lia Toledo
of Controlled Trials up to August 2012.
Damasceno, MD, PhD
Study Selection Eligible studies evaluated use of lower vs higher tidal volumes in patients without ARDS at onset of mechanical ventilation and reported lung injury devel- Marcus J. Schultz, MD, PhD
• 47/1113 Low Vt vs 38/1090 High Vt tổn thương phổi.
RR = 0,33 (0,23 – 0,41). NNT = 11
• Tỷ lệ tử vong ở nhóm bệnh nhân Low Vt giảm
RR =
is a life-saving strategy
in patients with acute
is a life-saving
strategy(0,46 – 0,89). NNT = 23
0,64
respiratory failure. Howin patients with acute
ever, unequivocal evidence suggests
respiratory failure. Howthat mechanical ventilation has the
ever, unequivocal•evidence
suggests
Tần
suất
viêm
phổi
và
xẹp
phổi
ở
nhóm
Vt
giảm
potentialLow
to aggravate
and precipitate
that mechanical ventilation has the
lung injury. In acute respiratory dispotential to aggravate and precipitate
tress syndrome (ARDS), and in a
RR
=
0,45
(0,22
–
0,92
).
NNT
=
26
lung injury. In acute respiratory dismilder form of ARDS formerly known
M
ECHANICAL VENTILATION
1
tress syndrome (ARDS), and in a
milder form of ARDS formerly known
as acute lung injury (ALI),2 mechanical ventilation can cause ventilatorassociated lung injury. Ventilatorassociated lung injury is a frequent
complication in critically ill patients
opment, overall mortality, pulmonary infection, atelectasis, and biochemical alterations.
Data Extraction Three reviewers extracted data on study characteristics, methods,
and outcomes. Disagreement was resolved by consensus.
M
ECHANICAL VENTILATION
Data Synthesis Twenty articles (2822 participants) were included. Meta-analysis using
a fixed-effects model showed a decrease in lung injury development (risk ratio [RR], 0.33;
95% CI, 0.23 to 0.47; I2, 0%; number needed to treat [NNT], 11), and mortality (RR,
0.64; 95% CI, 0.46 to 0.89; I2, 0%; NNT, 23) in patients receiving ventilation with lower
tidal volumes. The results of lung injury development were similar when stratified by
1
the type of study (randomized vs nonrandomized) and were significant only in randomized trials for pulmonary infection and only in nonrandomized trials for mortality. Metaanalysis using a random-effects model showed, in protective ventilation groups, a lower
incidence of pulmonary infection (RR, 0.45; 95% CI, 0.22 to 0.92; I2, 32%; NNT, 26), as acute lung injury (ALI),2 mechanilower mean (SD) hospital length of stay (6.91 [2.36] vs 8.87 [2.93] days, respectively; cal ventilation can cause ventilatorstandardized mean difference [SMD], 0.51; 95% CI, 0.20 to 0.82; I2, 75%), higher mean associated lung injury. Ventilator(SD) PaCO2 levels (41.05 [3.79] vs 37.90 [4.19] mm Hg, respectively; SMD, −0.51; 95%
associated lung injury is a frequent
CI, −0.70 to −0.32; I2, 54%), and lower mean (SD) pH values (7.37 [0.03] vs 7.40 [0.04],
2
respectively; SMD, 1.16; 95% CI, 0.31 to 2.02; I , 96%) but similar mean (SD) ratios of complication in critically ill patients
PaO2 to fraction of inspired oxygen (304.40 [65.7] vs 312.97 [68.13], respectively; SMD, receiving mechanical ventilation, and
2
Context Lu
has been foun
drome (ARDS
patients who
Objective T
proved outco
Data Source
of Controlled
Study Selec
tients without
opment, over
Data Extrac
and outcome
Data Synthe
a fixed-effects
95% CI, 0.23
0.64; 95% CI,
tidal volumes
the type of stu
ized trials for p
analysis using
incidence of p
lower mean (S
standardized m
(SD) PaCO2 lev
CI, −0.70 to −
respectively; S
PaO2 to fractio
0.11; 95% CI
did not influe
LOW TIDAL VOLUME
CONS
Tác giả
Thiết kế
So sánh
Kết cục
Fernandez
2014
RCT
28 BN
10 vs 6 ml/kg
Khơng thay đổi biomarker
(Neutrophil elastase,
Clara cell) tổn thương
phổi/60’ thơng khí
Wrigge
2004
RCT
12 – 15 +
PEEP = 0
vs 6 ml/kg+
PEEP = 10
Không khác biệt oxy máu
động mạch,TNF alpha,
IL1, IL6, IL8a, IL 12 / 3
giờ thơng khí
• Kallet 2001,2006: Bất đồng bộ bệnh nhân – máy thở,
nguy cơ xẹp phổi
• Lipshutz AK and Gropper (2013): Yếu cơ do thuốc dãn cơ
LOW TIDAL VOLUME
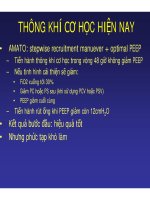
Nghiên cứu PreVENT
LOW TIDAL VOLUME
Figure. Estimates of the Effect of Low vs Intermediate Tidal Volume Ventilation Strategies in Subgroups Defined Post Hoc in the PReVENT Trial
Subgroups
Low Tidal Volume
Intermediate Tidal Volume
Ventilator-Free
Days,a Mean
(SD)
No.
Ventilator-Free
Days,a Mean
(SD)
No.
Nghiên cứu PreVENT
Favors Intermediate
Tidal Volume
Mean Difference
(95% CI)
Favors Low
Tidal Volume
P Value
Cardiac arrest
Yes
15.2 (12.4)
110
15.1 (12.4)
120
–0.00 (–3.17 to 3.29)
No
15.2 (11.3)
367
15.6 (11.1)
364
–0.38 (–2.02 to 1.25)
Yes
12.0 (11.7)
50
14.2 (10.8)
46
–2.20 (–5.46 to 1.06)
No
16.0 (11.4)
427
15.7 (11.6)
438
–0.25 (–1.38 to 1.89)
.80
Sepsis
.17
Postoperative ventilation
Yes
17.7 (11.1)
82
17.8 (10.8)
79
–0.08 (–3.26 to 3.09)
No
14.6 (11.6)
395
15.0 (11.5)
405
–0.38 (–2.01 to 1.25)
Higher
14.0 (11.4)
292
14.2 (11.4)
290
–0.19 (–2.06 to 1.66)
Lower
17.0 (11.6)
185
17.3 (11.3)
194
–0.27 (–2.61 to 2.07)
.87
Risk of ARDSb
.96
Pneumonia
Yes
13.3 (11.2)
77
11.7 (10.6)
77
1.56 (–1.94 to 5.08)
No
15.6 (11.6)
400
16.2 (11.5)
407
–0.58 (–2.18 to 1.01)
Yes
17.4 (11.2)
39
16.1 (12.2)
39
1.30 (–4.02 to 6.64)
No
15.0 (11.6)
438
15.4 (11.4)
445
–0.41 (–1.93 to 1.11)
.29
Airway protection
.53
Cardiac failure
Yes
15.4 (11.2)
28
18.4 (12.3)
17
–2.93 (–10.39 to 4.53)
No
15.2 (11.6)
449
15.4 (11.4)
467
–0.18 (–1.68 to 1.31)
.45
Head trauma or brain surgery
Yes
14.3 (12.0)
25
14.5 (10.5)
31
–0.18 (–6.32 to 5.95)
No
15.3 (11.6)
452
15.6 (11.5)
453
–0.29 (–1.80 to 1.21)
.97
Aspiration
Yes
14.1 (11.6)
20
14.9 (11.7)
24
–0.80 (–5.41 to 3.79)
No
15.3 (11.6)
457
15.5 (11.4)
460
–0.23 (–1.78 to 1.32)
All patients
.81
–0.27 (–1.74 to 1.19)
–6
–5
–4
–3
–2
–1
0
1
2
Mean Difference (95% CI)
3
4
5
6
LOW TIDAL VOLUME
Nghiên cứu PreVENT
• Phân nhóm trong 3 ngày đầu
– Ngày 0: 5,9 vs 9,1 ml/Kg
– Ngày 1: 6,6 vs 9,3 ml/Kg
– Ngày 2: 7,4 vs 9,1 ml/Kg
(p <0,001)
• Sau ngày đầu phần lớn chuyển sang PSV,
khó kiểm sốt Vt
• Miss 26 %, Khơng đồng ý 11 %
à Thơng khí 6 – 8 ml/kg.
HIGH PEEP
Tác giả
Thiết kế
So sánh
Kết cục
Manzano
2008
RCT
131 BN
5-8 cmH2O vs
0 cmH2O
Tử vong giống nhau
VAP thấp hơn ở PEEP cao
RR = 0,37 (0,15 – 0,84)
PROVE
Ary Serpa
Neto 2016
Metaanalysis
0 – 10 lower
Không thay đổi
PEEP vs 5 – 30 Tử vong, thời gian thở máy,
higher PEEP
ARDS hoặc viêm phổi
Futier E
2013
RCT
400 BN
10 – 12ml/kg +
No PEEP vs 6
– 8 ml/kg +
PEEP 6 - 8
Tổn thương phổi và ngoài
phổi RR = 0,4 (0,24 – 0,68)
Servegnini
2013
RCT
58 BN
T > 2h
9 ml/kg +
PEEP 0 vs 7
PEEP 10
CN hô hấp, oxy hoá máu
động mạch, X quang tốt
hơn ở bệnh nhân PEEP cao
Intensive Care Med
DOI 10.1007/s00134-016-4309-4
WHAT’S NEW IN INTENSIVE CARE
What’s new in mechanical ventilation
in patients without ARDS: lessons from the
PBW at a same ARDS
PEEP level
was associated
literature
Atelectasis
VILI
incidence of ARDS [5]. Two recent indi1,2,3
4*
Atelecto-trauma
(Volo-baro trauma )
mor bidity risk
mor bidity risk
Ary Serpa
Neto andthe
Samir
Jaber
data meta-analyses
confirmed
benefit
Lung infecƟon
Lung infecƟon
Hemodynamic side effects
entilation in ICU©patients
without
ARDS
[9,
2016 Springer-Verlag Berlin Heidelberg and ESICM
the use of lower Li
VT cs
did 2015
not increase sedapotentially damage the lungs and produce air leaks, and
Introduction
hich is cited as one
of the main2012
arguments
Gurudant
these lesions,OpƟmal
termed VT
‘barotrauma’, were believed to
The
incidence
of
acute
respiratory
distress
syndrome
.
e of lower VT [10].
(ARDS) varies greatly across the world [1], and its impact be the most relevant in the pathogenesis of ventilatorBellamy
the outcomeatelectasis
of 2006
critically ill patients
lower VT couldon
promote
even remains signifi- induced lung injury (VILI) for several years [7]. More
cant [1]. The publication of the ARMA trial [2] demon- recently, some studies showed, in animals ventilated
nger duration ofstrated
ventilation,
whichstrategy
could
à
U
that Shape
a lung protective
of ventilation, using with various VT but at similar airway pressures,
VTthat
Very lowitVT
< 3high
ml/kg
was
VT and not high airway pressures, that proa tidalof
volume
(VT)with
of 6 ml/kg
o use higher levels
PEEP
the predicted
aim body weight
from
then
(PBW), decreased mortality in patients with ARDS,
and duced
High VTand
> 10
ml/kg
(without
PEEP)VILI. This was called ‘volutrauma’
g closely similarledend
inspiratory
pressure.
to the
widespread, albeit
not universal, use of lung on researchers considered this more important than
barotrauma [7]. Meanwhile, investigators started to take
protective
strategies
in this group
of patients.
Ts have tested the
impact
of PEEP
in critiinterest in the beneficial effects of positive end
Recent studies suggest that the incidence of ARDS is Atelectasis
VILI expirats without ARDS.decreasing
In one[3,RCT
in patients at
tory
pressure
(PEEP)
in
the
prevention
of
VILI.
Use of)
4] and that this reduction is believed to
Atelecto-trauma
(Volo-baro trauma
too
low
levels
of
PEEP,
or
no
PEEP,
was
associated
with
be a result ofwith
advances
in hospital
practice
and
numerS, mechanical ventilation
8 cmH
O
of
Lung
infecƟon
2
Lung infecƟon
from repetitive
ous quality improvement initiatives [4]. These advances lung injury, and this was thought to result
Hemodynamic
side
effects
prevent the development
of this syndrome
included general quality improvement initiatives (i.e. opening and closing of lung tissue that collapses at the
no PEEP [11]. The
other
RCTtimely
showed
thatand resuscitation) end of expiration, a phenomenon called ‘atelectrauma’ 0
infection
control,
antibiotics
and also specific
critical care protocols
of ventilator-associated
pneumonia
was such as the use [7].The results of
OpƟmal PEEP
the Landmark ARMA trial confirmed
of protective ventilation in critically ill patients without
ents ventilated with
levels of PEEP
that VILI was not just an interesting experimental entity
ARDS higher
[5, 6].
Since the majority of the patients undergoing mechani- but was also an important clinical problem [2]. Indeed,
cal ventilation do not have ARDS, the number of stud- VILI is not just a problem in patients with ARDS but
PEEP
ies focusing on strategies of ventilation in this group of also in critically ill patients receiving mechanical ventilaARDS [4–7], and there has been a parapatients has been increasing in recent years, both Very
in surlow tion
PEEPbut
< 3without
cmH2O
nts
High PEEP > 10 cmH2O
gical and non-surgical areas. The purpose of this paper is digm shift from treating ARDS to prevention of ARDS in
complications, to especially
postoperative
review the recent
evidence in mechanical ventilation response to this scenario [5, 6, 8].
LOW DRIVING PRESSURE
- Quan sát tiến cứu
- 720 bệnh nhân
- 2 khoa ICU tại Hà Lan
- 4 nhóm
I (P/F ≥ 300 mm Hg; ΔP < 15 cm H2O)
II (P/F < 300 mm Hg; ΔP < 15 cm H2O)
III (P/F ≥ 300 mm Hg; ΔP ≥ 15 cm H2O)
IV (P/F < 300 mm Hg; ΔP ≥ 15 cm H2O)
- Outcome: Tử vong trong 90 ngày.
Sahetya et al. Critical Care
(2019) 23:367
/>
RESEARCH
LOW DRIVING PRESSURE
Open Access
Association between hospital mortality and
inspiratory airway pressures in mechanically
ventilated patients without acute
respiratory distress syndrome: a
prospective cohort study
Sarina K. Sahetya1, Christopher Mallow1, Jonathan E. Sevransky2, Greg S. Martin2,3, Timothy D. Girard4,
Roy G. Brower1, William Checkley1* and Society of Critical Care Medicine Discovery Network Critical Illness
Outcomes Study Investigators
THIẾT KẾ NGHIÊN CỨU
Abstract
Background: Higher inspiratory airway pressures are associated with worse outcomes in mechanically ventilated
patients with the acute respiratory distress syndrome (ARDS). This relationship, however, has not been well
investigated in patients without ARDS. We hypothesized that higher driving pressures (ΔP) and plateau pressures
(Pplat) are associated with worse patient-centered outcomes in mechanically ventilated patients without ARDS as
well as those with ARDS.
• Pplateau và Driving Pressure à kết cục bệnh nhân ARDS và
non
– collected
ARDS?
Methods:
Using data
during a prospective, observational cohort study of 6179 critically ill participants
enrolled in 59 ICUs across the USA, we used multivariable logistic regression to determine whether ΔP and Pplat at
enrollment
were associated
with tiến
hospital mortality
among 1132 mechanically ventilated participants. We stratified
• Quan
sát
cứu
analyses by ARDS status.
Results:
Participants
without
ARDS (n =1132
822) had lower
average severity
of illness scores and lower hospital
• 59
ICU
Mỹ,
bệnh
nhân
mortality (27.3% vs. 38.7%; p < 0.001) than those with ARDS (n = 310). Average Pplat (20.6 vs. 23.9 cm H O;
p < 0.001), ΔP (14.3 vs. 16.0 cm H O; p < 0.001), and positive end-expiratory pressure (6.3 vs. 7.9 cm H O; p < 0.001)
• lower
822
Non
- ARDS,
ARDS
were
in participants
without
whereas average tidal volumes (7.2 vs. 6.8 mL/kg PBW; p < 0.001) were
2
2
2
higher. Among those without ARDS, higher ΔP (adjusted OR = 1.36 per 7 cm H2O, 95% CI 1.14–1.62) and Pplat
(adjusted OR = 1.42 per 8 cm H2O, 95% CI 1.17–1.73) were associated with higher mortality. We found similar
relationships with mortality among those participants with ARDS.
Conclusions: Higher ΔP and Pplat are associated with increased mortality for participants without ARDS. ΔP may
be a viable target for lung-protective ventilation in all mechanically ventilated patients.
Infectious
(26.9)
Association
between hospital mortality221and
Gastrointestinal
122 (14.8)
inspiratory
airway pressures in mechanically
Trauma
61 (7.4)
ventilated
patients without acute
Endocrine
38 (4.6)
respiratory
distress syndrome: a
Other
134 (16.3)
prospective
cohort study
Sarina
K. Sahetya1, Christopher Mallow1, Jonathan E. Sevransky2, Greg S. Martin2,3, Timothy
Girard4,
Sepsis
261D. (31.8)
Roy G. Brower1, William Checkley1* and Society of Critical Care Medicine Discovery Network Critical Illness
Pneumonia
250 (30.4)
Outcomes
Study Investigators
ĐẶC ĐIỂM DÂN SỐ
APACHE II
Abstract
20.2 (7.4)
SOFA
(4–9) ventilated
Background: Higher inspiratory airway pressures are associated with worse outcomes in6mechanically
patients with the acute respiratory distress syndrome (ARDS). This relationship, however, has not been well
investigated
in patients without ARDS. We hypothesized that higher driving pressures (ΔP)
and plateau
pressures
PaO
255.6
(150.7)
2/FiO2
(Pplat) are associated with worse patient-centered outcomes in mechanically ventilated patients without ARDS as
well as those with ARDS.
Compliance respiratory system
39.6 (28.2)
Methods: Using data collected during a prospective, observational cohort study of 6179 critically ill participants
enrolled in 59 ICUs across the USA, we used multivariable logistic regression to determine whether ΔP and Pplat at
Plateau
(6.5)We stratified
enrollment pressure
were associated with hospital mortality among 1132 mechanically ventilated 20.6
participants.
analyses by ARDS status.
Driving
pressure
(6.0)
Results: Participants
without ARDS (n = 822) had lower average severity of illness scores 14.3
and lower
hospital
mortality (27.3% vs. 38.7%; p < 0.001) than those with ARDS (n = 310). Average Pplat (20.6 vs. 23.9 cm H2O;
p < 0.001), ΔP (14.3 vs. 16.0 cm H2O; p < 0.001), and positive end-expiratory pressure (6.35vs.(5–8)
7.9 cm H2O; p < 0.001)
PEEP
were lower in participants without ARDS, whereas average tidal volumes (7.2 vs. 6.8 mL/kg PBW; p < 0.001) were
1.14–1.62)
higher. volume
Among those(mL/kg
without ARDS,
higher ΔP (adjusted OR = 1.36 per 7 cm H2O, 95% CI7.2
Tidal
PBW)
(1.21)and Pplat
(adjusted OR = 1.42 per 8 cm H2O, 95% CI 1.17–1.73) were associated with higher mortality. We found similar
relationships with mortality among those participants with ARDS.
Hospital
LOS
18 (10–30)
Conclusions: Higher ΔP and Pplat are associated with increased mortality for participants without ARDS. ΔP may
be a viable target for lung-protective ventilation in all mechanically ventilated patients.
ICU
LOS
Keywords: Driving pressure, Mechanical ventilation, Acute respiratory failure, ARDS
10 (5–17)
Ventilator days
7 (3–14)
Mortality
224 (27.3)
Fig. 3 Cumulative distribution of tidal volume and PEEP by ARDS status. *p value for a difference in means
ARDS isAssociation
< 0.001. **p valuebetween
for a difference
in means ofmortality
PEEP for ARDSand
vs. non-ARDS is < 0.001
hospital
inspiratory airway pressures in mechanically
ventilated patients without acute
respiratory distress syndrome: a
prospective cohort study
Sarina K. Sahetya1, Christopher Mallow1, Jonathan E. Sevransky2, Greg S. Martin2,3, Timothy D. Girard4,
Roy G. Brower1, William Checkley1* and Society of Critical Care Medicine Discovery Network Critical Illness
Outcomes Study Investigators
KẾT QUẢ (tử vong)
Table 2 Odds of hospital mortality from multivariable logistic regression
Abstract
Non-ARDS
ARD
a
Background: Higher inspiratory airway pressures are associated
with worse outcomes
OR
95%inCImechanically ventilated p value
patients with the acute respiratory distress syndrome (ARDS). This relationship, however, has not been well
investigated in patients without ARDS.
We hypothesized that higher driving pressures (ΔP) and plateau pressures
Driving pressure
(per 7 cm H2O)bpatient-centered
1.36
1.14–1.62
< 0.001
(Pplat) are associated with worse
outcomes in mechanically ventilated patients without ARDS as
well as those with ARDS.
b
Plateau pressure
(per
8
cm
H
O)
1.42
1.17–1.73
< 0.001
2
Methods: Using data collected during a prospective, observational cohort study of 6179 critically ill participants
enrolled in 59 ICUs across the USA, we used multivariable logistic regression to determine whether ΔP and Pplat at
Age (per 5enrollment
years) were associated with hospital mortality among
1.051132 mechanically ventilated
0.98–1.11
participants. We stratified 0.125
analyses by ARDS status.
PEEP (per 1Results:
cm H
0.16
Participants
without ARDS (n = 822) had lower1.05
average severity of illness0.98–1.11
scores and lower hospital
2O)
mortality (27.3% vs. 38.7%; p < 0.001) than those with ARDS (n = 310). Average Pplat (20.6 vs. 23.9 cm H2O;
< 0.001),
ΔP (14.3 vs. 16.0 cm H2O; p < 0.001), and positive
(6.3 vs. 7.9 cm H2O; p < 0.001)
APACHE II p(per
1 point)
1.08 end-expiratory pressure
1.04–1.11
< 0.001
were lower in participants without ARDS, whereas average tidal volumes (7.2 vs. 6.8 mL/kg PBW; p < 0.001) were
95% CI 1.14–1.62) and Pplat
higher.
OR = 1.36 per 7 cm H2O,
Vasopressor
useAmong those without ARDS, higher ΔP (adjusted
1.52
1.06–2.16
0.02
(adjusted OR = 1.42 per 8 cm H2O, 95% CI 1.17–1.73) were associated with higher mortality. We found similar
relationships with mortality among those participants with ARDS.
Sepsis
1.12
0.77–1.62
Conclusions: Higher ΔP and Pplat are associated with increased mortality for participants without ARDS. ΔP may
be a viable target for lung-protective ventilation in all mechanically ventilated patients.
0.56
ORa
1.63
1.74
1.09
1.12
1.08
1.02
1.03
Abbreviations: ARDS acute respiratory distress syndrome, APACHE Acute Physiologic and Chronic Health Evaluation, PEE
odds ratio Keywords: Driving pressure, Mechanical ventilation, Acute respiratory failure, ARDS
Estimates for covariates are derived from the driving pressure model. The plateau pressure model included the same
a
Odds ratio adjusted for age, sex, PEEP, APACHE II, vasopressor use, sepsis, hospital volume, and ICU category
b
Odds ratios for driving pressure and plateau pressure are scaled to IQRs
PHÒNG MỔ
Tác giả
Thiết kế
Dân
số
So sánh
IMPROVE
RCT
400 BN
Phẫu 10 – 12 ml/kg +
thuật PEEP =0 vs
6 – 8 ml/kg + PEEP
=6 – 8
Mean T = 200 mins
Sutherasan
2014
Review
Phẫu 9ml/kg
Metanalysis thuật
tăng biến chứng hô hấp,
yếu tố độc lập trong suy
đa cơ quan
Hypoxemia, BC phổi, T
thở máy, Tử vong
PROVHIO
trial
2014
RCT
900 BN
Châu Âu+
Mỹ
Không khác biệt biến
chứng ở High vs Low
PEEP
Phẫu PEEP
thuật 12( 12 ; 12) vs 2 (0 ;
2)
Mean T = 200 mins
Kết cục
Low Vt ít biến chứng hô
hấp, nhiễm trùng, shock,
tử vong hơn.
Huyền thoại “500ml” à CDC: 10 % nam , 85 % nữ có Vt > 8 ml/kg
CẤP CỨU
• Nguồn nhập khoa HSCC 42,5 %
• Đặt nội khí quản tại cấp cứu 6,8 – 8 % à ARDS 14 –
27,5 %.
• Huyền thoại “500ml”
• 10% bệnh nhân thở máy non-ARDS được điều chỉnh
máy thở.
• 42 % bệnh nhân nhận cùng thơng số khi chuyển ICU.
• 28 % khơng đổi trong 24 giờ.
• Stolze và cs: sử dụng Vt ở trước viện à ảnh hưởng
Vt nhập viện 7,06 lần
anuscript
Lung-protective ventilation initiated in the emergency
department (LOV-ED): a quasi-experimental, before-after trial
Brian M. Fuller, MD, MSCI,
Departments of Emergency Medicine and Anesthesiology, Division of Critical Care, Washington
University School of Medicine in St. Louis, St. Louis, MO 63110, USA
Nicholas M. Mohr, MD, MS,
• 1192Departments
BN trước
can thiệp
of Emergency Medicine and Anesthesiology, Division of Critical Care, Roy J. and
Lucille A. Carver College of Medicine, University of Iowa, 200 Hawkins Drive, 1008 RCP, Iowa
• 513 City,
BNIAsau
can thiệp
52242, USA
–
–
–
–
Author Manuscript
Author Manuscript
Ian T. Ferguson, MPH,
al.
School of Medicine Fuller
and etMedical
Science, University College Dublin, Dublin 4, Ireland
Vt thấp à bảo vệ phổi
Anne M. Drewry, MD, MSCI,
PEEP
tránhofxẹp
phổi
Department
Anesthesiology,
Division of Critical Care Medicine, Washington University School
of Medicine
St. Louis,
St. Louis, MO 63110, USA
Tránh
tăng inoxy
quá mức
Đầu
cao
Christopher
Palmer, MD,
Brian T. Wessman, MD,
Departments of Emergency Medicine and Anesthesiology, Division of Critical Care, Washington
Figure 3. Distribution of emergency department tidal volume
University School of Medicine in St.
Louis,
Louis, in
MO
63110, USA
There
was St.
an increase
lung-protective
ventilation in the ED associated with the
Author Manuscript
Author Manuscript
Departments of Emergency Medicine and Anesthesiology, Division of Critical Care, Washington
University School of Medicine in St. Louis, St. Louis, MO 63110, USA
intervention (47.8% to 96.2%).
Enyo Ablordeppey, MD, MPH,
ED: emergency department; PBW: predicted body weight
Departments of Emergency Medicine and Anesthesiology, Division of Critical Care, Washington
University School of Medicine in St. Louis, St. Louis, MO 63110, USA
anuscript
2
Lung-protective ventilation Table
initiated
in the emergency
Ventilator
variables in the emergency
department
department
(LOV-ED):
a quasi-experimental, before-after trial
*
Group
Intervention Group (n=
Odds Ratio or Between-Group
Brian M. Fuller, MD, MSCI, Pre-intervention
(n= 1,192)
513)
Difference (95% CI)
Departments of Emergency Medicine and Anesthesiology, Division of Critical Care, Washington
Tidal volume,
mL
University
School of Medicine in St. Louis, St. Louis, MO 63110, USA
Median (IQR)
500 (500–550)
420 (370–470)
Author Manuscript
Ian T. Ferguson, MPH,
Mean (SD)
515.7 (71.6)
422.0 (71.5)
−93.7 (−99.5 to −87.8)
School of Medicine and Medical Science, University College Dublin, Dublin 4, Ireland
Tidal volume, mL/kg PBW
Nicholas M. Mohr, MD, MS,
8.1 (7.3–9.1)
6.3 (6.0–6.7)
Departments of Emergency Medicine and Anesthesiology, Division of Critical Care, Roy J. and
Mean (SD)
8.3 (1.5)
(0.8)
(−1.9 to −1.7)
Lucille A. Carver College of Medicine,
University of Iowa,6.4200
Hawkins Drive,−1.8
1008
RCP, Iowa
PEEP City, IA 52242, USA
Median (IQR)
Median
(IQR)
Anne
5 (5–5)
5 (5–8)
M. Drewry, MD, MSCI,
Mean Department
(SD)
5.4 (1.5)of Critical Care Medicine,
6.5 (2.5)
(0.9 to 1.3) School
of Anesthesiology, Division
Washington1.1
University
of Medicine in St. Louis, St. Louis, MO 63110, USA
Respiratory rate
Median
(IQR)
Christopher
Author Manuscript
14 (12–16)
20 (20–24)
Palmer, MD,
of Emergency Medicine
and Anesthesiology,
of Critical Care,
Washington
Mean Departments
(SD)
15.3 (3.5)
20.9 Division
(3.8)
5.6 (5.3 to
5.9)
University School of Medicine in St. Louis, St. Louis, MO 63110, USA
FiO2
Brian
Median
(IQR)
T. Wessman, MD,
80 (50–100)
40 (40–60)
of Emergency Medicine
and Anesthesiology,
Division of Critical
Care,
Mean Departments
(SD)
75.0 (25.9)
53.4 (21.7)
−21.6
(−23.5Washington
to −19.8)
University School of Medicine in St. Louis, St. Louis, MO 63110, USA
Head-of-bed elevation, n (%)
989 (39.4)
704 (92.6)
19.4 (14.6–25.7)
Enyo Ablordeppey, MD, MPH,
Lung protective
ventilation, of
n (%)
1202 (47.8)
731 (96.2)
(21.8–64.7)
Departments
Emergency Medicine
and Anesthesiology,
Division of Critical 37.6
Care,
Washington
University School of Medicine in St. Louis, St. Louis, MO 63110, USA
Manuscript
Lung-protective
ventilation initiated in the emergency
Table
4
Table 4
department (LOV-ED): a quasi-experimental, before-after trial
Results of outcome
analyses
Brian M. Fuller,
MD, MSCI,
Departments of Emergency Medicine and Anesthesiology, Division of Critical Care, Washington
University School of Medicine in St. Louis, St. Louis, MO 63110, USA
Author Manuscript
After Matching
Matching
Before
Ian T. Ferguson, MPH,
School of Medicine and Medical Science, University College Dublin, Dublin 4, Ireland
Nicholas M. Mohr, MD, Pre-intervention
MS,
*OR
OR or Between-Group
InterventionGroup
Group
Intervention
or or
Between-Group
aOR
Between-Group
Departments
of
Emergency
Medicine
and
Anesthesiology,
Division
of
Critical
Care,
Roy
J.
and
Difference (95% CI)
Group(n=
(n=1,192)
490)
(n= 513)
490)
Group
(n=
Difference
Difference(95%
(95%CI)
CI)
Lucille A. Carver College of Medicine, University of Iowa, 200 Hawkins Drive, 1008 RCP, Iowa
City, IA 52242, USA
Pr
Gr
0.48 (0.33–0.69)
71 (14.5)
36 (7.4)
(7.4)
0.47(0.33–0.69)
(0.31–0.71)
Primary
composite
(14.3)
38
0.48
Anne M. Drewry, MD, MSCI,171
0.37 (0.23–0.58)
53Division
(10.8)
20Washington
(4.1) University School 0.37
0.35(0.23–0.58)
(0.21–0.60)
outcome,
n (%)
130
(10.9)
22
(4.3)
Department of Anesthesiology,
of Critical Care Medicine,
of Medicine in St. Louis, St. Louis,
63110, USA
•ARDS
86
(7.2)
23
0.60
0.60
(0.38–0.97)
37 MO
(7.6)
23 (4.5)
(4.7)
0.60(0.38–0.97)
(0.35–1.03)
•VACs Christopher Palmer, MD,
Departments of Emergency Medicine and Anesthesiology, Division of Critical Care, Washington
University School of Medicine in St. Louis, St. Louis, MO 63110, USA
Author Manuscript
Ventilator-free
days
2.17 (1.06 to 3.29)
16.0
14.7 (11.4)
(11.7)
18.2
18.4 (10.5)
(10.4)
2.17
3.69(1.06
(2.30toto3.29)
5.07)
Brian T. Wessman, MD,
Departments of Emergency Medicine and Anesthesiology, Division of Critical Care, Washington
University School of Medicine in St. Louis, St. Louis, MO 63110, USA
Hospital-free
0.87
(−0.09 todays
1.84)
10.8
(9.6)
9.4 (9.5)
11.6
11.7 (9.2)
(9.2)
0.87
2.38(−0.09
(1.21toto1.84)
3.55)
Enyo Ablordeppey, MD, MPH,
ICU-free
days
15.0
15.8
0.77
0.77
(−0.30
toDepartments
1.83) of Emergency Medicine
13.6 (10.8)
(11.1)
16.0(10.0)
(9.9)
2.36(−0.30
(1.04toto1.83)
3.68)
and Anesthesiology, Division of Critical Care, Washington
University School of Medicine in St. Louis, St. Louis, MO 63110, USA
Mortality,
n (%)
0.65 (0.51–0.83)
Jacob Keeperman, MD,
338
167 (28.4)
(34.1)
105
(20.5)
96 (19.6)
0.65
0.47(0.51–0.83)
(0.35–0.63)
Correspondence
M. Fuller.
primaryand
outcome
pulmonary outcome that combines the event rate for ARDS and VACs.
ateThe
for ARDS
VACs.wasto: aBriancomposite
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our
Author Manusc
customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of
the resulting proof before it is published in its final citable form. Please note that during the production process errors may be
discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
OR:distress
odds ratio;
CI: confidence
interval; aOR: adjusted
odds ratio;
acute
respiratory
distress syndrome; VAC: ventilat
ratory
syndrome;
VAC: ventilator-associated
condition;
ICU:ARDS:
intensive
care
unit
Meetings: Partial data from the implementation phase of this work was presented at the American Thoracic Society Conference on
May 17, 2016 in San Francisco, California. The results of the study will be presented as an oral abstract presentation (Star Research
Presentation) on January 22, 2017 in Honolulu, Hawaii for the Society of Critical Care Medicine 46th annual congress.
*
From
logistic
regression
modeling
(categorical
data)
and generalized
estimating equations negative binomial regression (con
ations
negative
binomial
regression
(continuous
data).
Summary Conflict
of Interest Statement:
All authors declare
that no conflicts
of interest exist.